Resources
Latest Posts
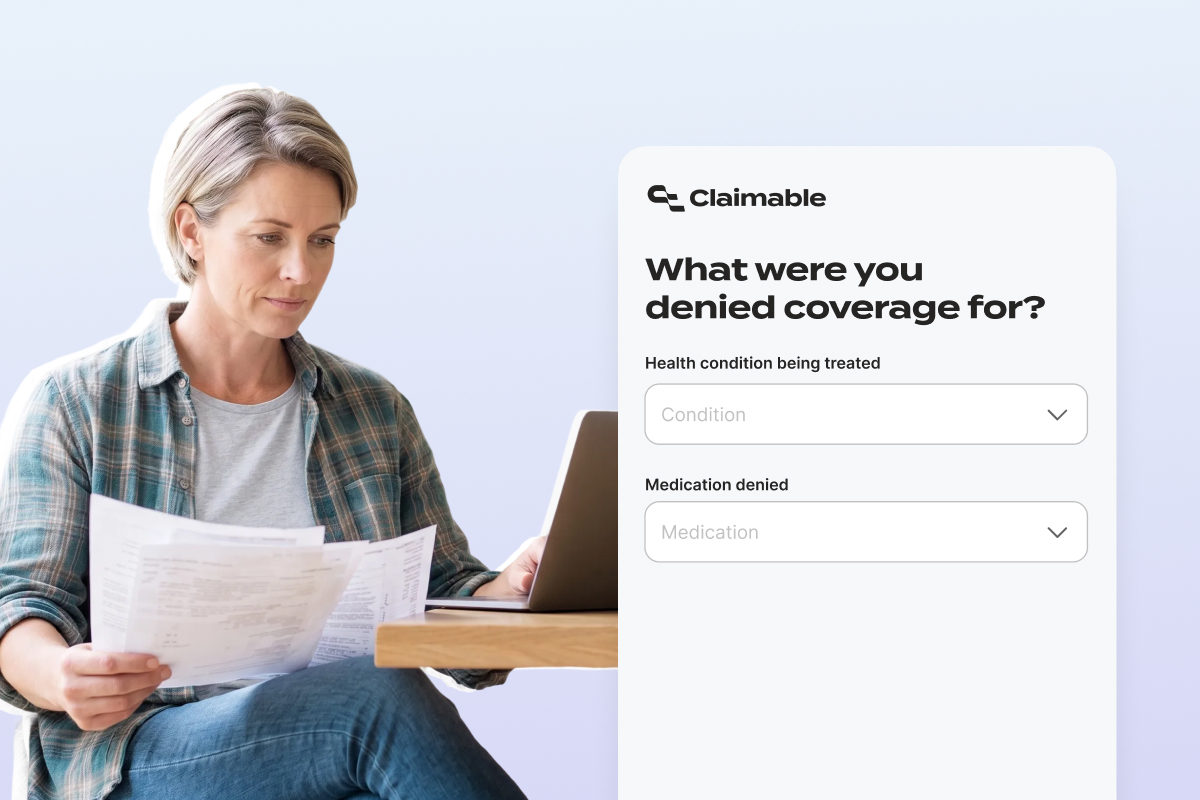
If you landed here, chances are you just got an insurance denial for a treatment you need — and when you came to Claimable for help, we told you we don't support your medication or condition yet.
We know how frustrating that is. You're already dealing with the stress of being denied care your doctor prescribed, and the system is putting up roadblocks at every turn. While we're sorry we can't help you today, we're still here to help break those barriers down.
In this post, we'll explain why we aren't available for every denial just yet – but more importantly, what you can still do to fight for the coverage you deserve.
Why We Don't Support Everything (Yet)
Every condition and medication on the Claimable platform has a fully validated appeal strategy behind it. Our team researches and pressure-tests specific clinical guidelines, laws, insurer policy language, and denial patterns, building them into the platform before we'll generate a single appeal for a patient. That research is what allows us to create strong, powerful appeals from millions of possible strategy combinations rather than producing a generic letter.
We take seriously that what we create could determine whether or not you get treatment. An appeal built on the wrong argument, a misapplied citation, or a legal standard that doesn't apply to your plan type can mean another denial. When winning an appeal can mean the difference between getting care and going without it, it's critical to us to make sure every appeal we support meets a high bar for accuracy and quality.
So we don't support everything – just yet. We're always adding support for more medications and conditions, and our hope is that someday soon, Claimable can be used to appeal every single denial in the American healthcare system (all 850 million of them!). But until that day comes, we're still here to help you get covered however we can.
What Makes a Strong Appeal
Whether you use Claimable, write your own appeal, or use another tool, the strongest appeals combine three things: your personal health story (how the denial is specifically affecting your life and function), clinical evidence (guidelines and studies from recognized medical societies that support your treatment), and policy and legal analysis (the specific plan provisions and laws that apply to your denial type and plan type). When all three work together, that's when denials are most likely to be overturned.
The specifics matter more than most people realize. A formulary exclusion denial and a medical necessity denial for the same medication require fundamentally different strategies: different clinical evidence, different legal arguments, even a different tone. A formulary appeal needs to demonstrate that no therapeutically equivalent alternative exists for you specifically, while a medical necessity appeal needs to dismantle the insurer's rationale for why your treatment isn't needed. The legal protections available to you depend on your plan type and state.
The TLDR? Getting it right is important. That's what we're built to do, and in the meantime, we've put together some resources to help.
What Can I Do Instead of Claimable?
The good news: you have the right to appeal regardless of whether Claimable supports your condition. That right comes with real protections most patients don't know about — mandated response timelines, multiple levels of review, and for most plan types, the right to an independent external review where someone outside your insurance company evaluates your case.
Here's where to start:
Download Our Sample Appeal Letter Template → Follows the three-pillar structure with prompts for your personal details, clinical evidence, and legal arguments.
10 Essential Patient Appeal Rights Every Patient Should Know →
Breaks down the specific legal protections you have when appealing a denial — including rights most patients don't know exist.
How to Get a Non-Formulary Drug Covered →
If your denial is formulary-related, this guide walks you through the exception request and appeal process step by step.
Why You Should Appeal Your Insurance Denial Yourself →
Patient appeals carry legal protections that provider appeals don't. This post explains why — and how to use that to your advantage.
Find Your State Department of Insurance →
Every state has one, and they exist to help people in your situation. They can tell you your exact review rights and intervene if your insurer isn't following the rules.
ProPublica's Claim File Helper →
Free tool that generates a letter requesting your claim file — the internal notes, correspondence, and records your insurer used when deciding to deny you.
HealthInsuranceAppeals.org →
Led by attorney D. Brian Hufford, this organization partners with law schools to provide free pro bono assistance to patients appealing health insurance denials.
Patient Advocate Foundation →
Offers case management for patients navigating insurance denials.
Ask your doctor's office about submitting a peer-to-peer review request or letter of medical necessity alongside your appeal. A patient appeal and a provider appeal working in parallel create pressure from two directions – and if one is denied, the other keeps going.
Thinking About Using ChatGPT or Another AI Tool?
We say: go for it. Using an AI tool to draft your appeal is far better than not appealing at all. But don't treat its output as final – AI language models make mistakes that aren't always obvious, and in an appeal, accuracy matters. This applies to general-purpose AI like ChatGPT and Gemini, as well as many broad insurance AI tools that build appeals off of general statements instead of specific medical information. Before you submit anything AI-generated:
Check that every clinical study cited actually exists. Search each one by title in PubMed or Google Scholar. AI tools routinely fabricate convincing-looking citations that aren't real, and a fabricated citation undermines your credibility with the reviewer.
Confirm that laws and regulations referenced are real and apply to your plan type. AI tools will cite statutes that don't exist or apply federal protections to plans they don't cover. Look up anything the tool references.
Make sure the appeal addresses your actual denial reason. Medical necessity, formulary exclusion, and step therapy denials each require fundamentally different arguments. If the tool argues the wrong one, the strongest evidence in the world won't matter.
Verify that clinical guidelines are current and from recognized medical societies. Outdated guidelines can work against you if the reviewer is using the current version.
Be careful with your personal health information.Your appeal will include sensitive medical details — your diagnosis, treatment history, medications, and how your condition affects your daily life. Before entering any of that into an AI tool, understand how that tool handles your data. Most general-purpose AI chatbots are not HIPAA-compliant, which means your health information may be stored, used for model training, or accessible in ways you didn't intend.
You might be thinking… isn't Claimable powered by AI? The difference is that our AI is purpose-built for insurance appeals. We use a human-in-the-loop model and multiple quality check gates that cross-reference our database for accuracy, strategy alignment, and argument soundness. Plus, we're HIPAA-certified and SOC 2 compliant: Your data is fully encrypted and handled under the same privacy standards your doctor's office is required to follow.
We're Adding Support for More Appeals All the Time
Our team is continually researching and validating appeal strategies for new conditions and medications. The 85+ medications we support today are growing – and our goal is to be there for every patient who needs to appeal a denial, no matter what treatment they've been denied.
If you'd like to be notified when we add support for your condition, sign up updates here. We'll let you know the moment we can help.
In the meantime: you have the right to appeal. The process is stacked against you on purpose — insurance companies count on the complexity being enough to make you walk away. Nearly half of patients do. But the ones who appeal, with the right evidence and the right arguments, overturn denials at dramatically higher rates than most people expect.
Your denial isn't the final answer. It's the first move in a process that's designed to have a next step. Take it.

Over 70% of patients referred to Claimable complete and submit an appeal, with more than 80% submitted same day
SAN FRANCISCO — Claimable today announced the debut of its enterprise patient access platform, purpose-built for pharmaceutical manufacturers, health systems, and access partners, including specialty pharmacies and patient support hubs.
The AI-powered platform extends patient access programs beyond prior authorization, automating the appeal layer that sits between a patient's prescription and coverage for their needed therapy. By integrating directly into existing patient support programs and revenue cycle operations, Claimable addresses the growing denial problem without adding headcount or replacing existing systems.
The Denial Crisis
Denials are now the leading cause of treatment delays and patient dropout in specialty care. Denial rates are rising 25% year over year as payers increasingly leverage AI to automate claim reviews. The support infrastructure most manufacturers and health systems rely on was built for a different era. Call centers, manual workflows, overstretched clinical staff, disconnected case management: none of it was designed to keep pace with AI-powered denials. As a result, 99% of denials are never challenged, and 46% of patients abandon treatment after a denial, leaving medically necessary therapies out of reach for millions.
Platform Scale and Results
Claimable covers more than 85 commonly restricted treatments spanning asthma, obesity, diabetes, autoimmune disorders, and rare pediatric diseases. The enterprise platform is already live across 10 programs supporting treatments used by over one million patients nationwide, where initial denial rates can reach 70%.
"Insurers have figured out how to use AI to deny care at scale, while everyone else is left trying to fight back one appeal at a time," said Warris Bokhari, MD, CEO and Co-Founder of Claimable. "The asymmetry is stark — denials are automated, but appeals are not, and that breakdown puts lives at stake. Patients are left to make impossible choices: delay treatment, pay out of pocket for medications that can cost more than $1,000 per month — or walk away from care altogether. We built Claimable to restore that balance of power, using AI so appeals move as fast as denials do, at the scale the problem demands."
Most denied patients receive no appeal support at all, and those who do wait days or weeks for a provider to prepare and file. By contrast, Claimable scales appeal support to every denied patient, cutting the time between denial and treatment initiation. More than 70% of patients referred to Claimable complete and submit an appeal, with more than 80% submitted the same day.
Across established conditions, Claimable has achieved success rates exceeding 80%, with denials overturned in under 10 days on average. To date, the platform has recovered more than $30 million in previously denied care, reducing treatment delays, improving patient retention, and saving access and clinical teams hours of administrative work per appeal.
How It Works
The process begins with flexible intake, allowing patients to enter through direct links, support team referrals, or API-based integrations with existing workflows. A guided, self-service experience allows most patients to build a personalized appeal in under 30 minutes.
Claimable's AI appeal engine generates a case-specific appeal by combining three layers of evidence: the patient's personal health narrative, a curated library of clinical studies and guidelines, and laws and health plan policies. Each appeal is matched to the exact treatment, condition, insurer, and denial reason, producing millions of bespoke strategy combinations.
Enterprise Capabilities
The platform also provides enterprise teams with a set of operational tools to support patients throughout the appeals process:
Enterprise operations console: centralized management layer supporting referral submission, document upload, real-time case tracking, and outcome visibility with role-based access controls.
Program dashboard: aggregate, de-identified reporting to continuously optimize access strategies, including denial patterns and outcomes, conversion, and engagement analytics.
Access content suite: branded landing pages, advocacy resources, training guides, call scripts, and email templates, all built to medical-legal review and compliance standards.
Security and Compliance
Security, governance, and safety oversight are native to the platform, including HIPAA-compliant hosting, SOC 2 Type II certification, consent management, audit trails, and AI-powered pharmacovigilance workflows that monitor patient-reported responses against FDA adverse event data.
Each enterprise deployment is assigned a named appeal specialist available to review escalated cases and adjust appeal approaches as payer behavior changes.
To learn more about how Claimable supports pharmaceutical manufacturers and health systems, visit getclaimable.com/for-pharma and getclaimable.com/for-health-systems.
About Claimable
Claimable is an intelligent patient access platform that closes the gap between the care patients are prescribed and the coverage they receive by challenging insurance denials at scale. Leveraging purpose-built AI and automation, the platform analyzes clinical research, policy details, appeals data, and patients' unique medical histories to generate and submit customized appeals in minutes. Available nationwide, the platform supports denials from all insurance providers, including Medicare and Medicaid. Claimable has been recognized by Fierce Healthcare's Fierce 15, Fast Company's World Changing Ideas, and TIME100 Health for its leadership in patient access innovation. Backed by Quiet Capital, Next Level Ventures, Walkabout VC, Great Oaks, and others, the company continues to push the boundaries of AI innovation in healthcare. To learn more, visit www.getclaimable.com.
Contact:
Emily Fox
press@getclaimable.com
Your neurologist prescribed Emgality because it’s the right preventive treatment for your migraines. Your health insurer decided otherwise. But an insurance denial isn’t the end of the conversation, and you have legal rights that most patients never exercise.
Emgality (galcanezumab-gnlm) is a calcitonin gene-related peptide (CGRP) monoclonal antibody, one of a class of injectable therapies specifically designed to prevent migraine attacks before they start. Unlike older preventive medications that were originally developed for other conditions and repurposed for migraines, Emgality was built from the ground up to target the CGRP pathway, a biological mechanism central to how migraines work. It received FDA approval in September 2018 for preventive treatment of migraine in adults and is also approved for episodic cluster headache.
Despite strong clinical evidence and more than 90% of commercial health plans including Emgality coverage on their formularies, actually getting that coverage activated is a different story. Most plans require prior authorization, and the majority demand that you try and fail two or more older preventive medications before they’ll approve a CGRP drug like Emgality. If you’re reading this, you’ve likely already hit that wall.
Here’s the reality insurance companies don’t advertise: fewer than 1% of denied claims are ever appealed. When patients do appeal with the right evidence, the results are dramatically different. At Claimable, over 80% of our appeals succeed in established conditions.
This guide explains exactly why Emgality gets denied, what makes these denials often medically unjustifiable, and how to build an appeal that wins, including the clinical arguments, documentation strategies, and legal protections that actually change outcomes.
Our physician-led team has built a database of over 4 million clinical studies, insurer policies, and legal standards to fight denials like yours. We know which arguments overturn Emgality denials, and we know the step therapy tactics insurers use to delay access to CGRP drugs.
Why Insurance Companies Deny Emgality Coverage
Before you do anything else, find the specific reason your insurer denied your prescription. The denial reason determines your entire appeal strategy, and using the wrong argument wastes time you don’t have.
The Step Therapy Problem: Months of Medication Roulette Before You Get What Actually Works
Most Emgality denials come down to one thing: step therapy. Your health insurer requires you to try and fail older, cheaper standard preventatives before they’ll approve a migraine-specific CGRP inhibitor, even when the leading medical society in headache medicine says that requirement is no longer clinically justified.
The medications insurers typically demand you try first weren’t designed for migraines at all. They’re repurposed therapies from other fields: beta-blockers originally developed for blood pressure and heart conditions (propranolol, metoprolol), antidepressants (amitriptyline, venlafaxine), and antiepileptic drugs (topiramate, valproate). Some of these drugs do help some patients, but the side effect profiles are significant, and the dropout rates tell the real story.
Consider topiramate, one of the most commonly required step therapy medications. In clinical trials for migraine prevention, approximately 25% of patients on the standard 100mg dose discontinued treatment due to adverse events. The most common reasons: paresthesia (tingling and numbness), fatigue, and difficulty with concentration and memory. These side effects are severe enough that patients often call topiramate “Dopamax” for its cognitive effects. Beta-blockers can cause fatigue, depression, and exercise intolerance. Antidepressants carry their own constellation of side effects including weight gain, dry mouth, and sedation.
Insurers know all of this. Step therapy isn’t a medical strategy. It’s a cost strategy. The older drugs are cheaper, and the insurer saves money for every month you spend trying medications that may not work and may make you feel worse.
The American Headache Society’s 2024 position statement directly challenges this approach. After reviewing more than a decade of clinical evidence and real-world experience, the AHS now recommends that CGRP inhibitors, including Emgality, should be considered a first-line option for effective migraine prevention, without requiring prior failure of other drug classes. The statement is unequivocal: the cumulative evidence for efficacy, safety, and tolerability of CGRP therapies is significantly greater than that for any established migraine preventive treatment.
When your insurer requires you to spend months cycling through medications with high discontinuation rates and substantial side effects before approving Emgality, they’re overriding the judgment of both your prescribing neurologist and the nation’s leading headache specialists.
The Most Common Emgality Denial Types
| Denial Type | What Your Letter Says | What It Actually Means | Best First Move |
|---|---|---|---|
| Step Therapy Required | “Must try preferred alternatives first” | Insurer wants proof you failed 2+ classes of older preventives | Document prior failures, side effects, or contraindications |
| Not Medically Necessary | “Does not meet medical necessity criteria” | Documentation was insufficient or key details were missing | Resubmit with comprehensive clinical evidence |
| Not on Formulary | “Drug not on preferred drug list” | Plan prefers a different CGRP medication | Request formulary exception with clinical rationale |
| Frequency Threshold Not Met | “Does not meet minimum migraine days” | Insurer says your migraine frequency doesn’t qualify | Document true migraine burden with headache diary |
| Incorrect Diagnosis Code | Varies | Wrong or incomplete ICD-10 code submitted | Work with prescriber to correct coding |
| Prior Authorization Expired | “Authorization no longer active” | Previous PA lapsed and needs renewal | Resubmit with updated treatment response data |
Step Therapy Required
This is the most common reason Emgality injections are denied. Insurers including Aetna, Anthem Blue Cross, Cigna, UnitedHealthcare, Blue Shield, and Humana all typically require documented failure of at least two classes of preventive medications before approving CGRP drugs. The specific requirements vary by plan, but the pattern is consistent: try the cheap options first, even if your doctor has already determined they’re not right for you.
“Failure” is defined more broadly than most patients realize, and that’s where your appeal leverage lives. You don’t need to prove a medication was completely useless. Any of the following counts: the drug didn’t reduce your migraine frequency enough, side effects or intolerances made the drug unbearable, you have a medical condition that contraindicates the drug (cardiovascular disease for beta-blockers, kidney stones for topiramate, pregnancy planning for valproate), or you had to discontinue for any documented medical reason. Prior medication trials from other doctors or previous insurers also count. You shouldn’t have to restart the failure clock every time your coverage changes.
Important: The AHS 2024 position statement specifically states that initiation of CGRP-targeting therapies should not require trial and failure of non-specific migraine preventive medication approaches. This is your strongest clinical argument in any step therapy appeal.
Not Medically Necessary
A medical necessity denial usually means the initial submission didn’t include enough clinical detail, not that your insurer made a careful medical judgment. Common documentation gaps for Emgality include: not specifying the number of migraine days per month, not providing a complete treatment history with specific drug names, dosages, durations, and outcomes, not documenting how migraines impact your ability to work and function, or not explaining why Emgality specifically is the right choice.
For Emgality, your prescriber’s documentation should establish your migraine diagnosis with the correct ICD-10 code, quantify your migraine burden (frequency, severity, and disability), list every prior preventive medication tried with specific reasons each was inadequate, and articulate the clinical rationale for choosing a CGRP monoclonal antibody.
Not on Formulary / Non-Preferred Brand
Some health insurance plans prefer a different injectable CGRP medication, often Aimovig (erenumab), Ajovy (fremanezumab), or Vyepti (eptinezumab), over Emgality. This is typically a pricing decision, not a clinical one. All four injectable CGRP drugs are effective preventive therapies, but they’re not interchangeable for every patient.
This matters for your appeal: Emgality and Ajovy work by binding the CGRP ligand (the protein itself), while Aimovig targets the CGRP receptor. These are meaningfully different mechanisms, and patients who don’t respond to one may respond well to another. If your insurer is asking you to switch to a preferred alternative, and you’ve already tried that medication without adequate results or your neurologist has a specific clinical reason for choosing Emgality, that’s a strong basis for a formulary exception.
The CONQUER trial specifically demonstrated that Emgality is effective in patients who have failed two to four prior preventive medication categories, meaning it has published evidence of working in exactly the population most likely to face insurance barriers.
Frequency Threshold Not Met
Most insurers require a minimum of 4 migraine days per month to qualify for Emgality coverage. If your denial cites this reason, it often means the documentation didn’t clearly establish your migraine frequency, not that you don’t actually meet the threshold. A detailed headache diary showing your true migraine burden, corroborated by your neurologist’s clinical assessment, is typically what’s needed to address this.
Keep in mind that many patients underreport migraine frequency in routine visits. If you experience 4 or more migraine days per month (the standard clinical threshold for considering preventive treatment), make sure that number is explicitly documented in your medical records.
Incorrect Diagnosis Code
Emgality coverage requires specific ICD-10 migraine diagnosis codes. Common codes that support Emgality prescriptions include: migraine without aura (G43.00, G43.01), migraine with aura (G43.10, G43.11), chronic migraine without aura (G43.709, G43.711), and migraine, unspecified (G43.90, G43.91). Using a general headache code like R51.9 (“headache, unspecified”) will almost certainly trigger a denial.
If your denial stems from a coding issue, this is often the simplest fix. Work with your prescriber’s office to verify and correct the submitted diagnosis code.
Prior Authorization Expired
Emgality typically requires reauthorization every 6 to 12 months. If your PA has lapsed, you’ll need to resubmit with updated documentation showing that the medication is still working, ideally including migraine diary data demonstrating continued response (a 50% or greater reduction in monthly migraine days is the standard clinical benchmark). Start the renewal process 30 to 45 days before your current authorization expires to avoid gaps in treatment.
How to Appeal an Emgality Denial: Step by Step
A denial is not a final answer. It’s the beginning of a process that patients are legally entitled to, and that works far more often than the insurance industry would like you to believe.
Step 1: Read Your Denial Letter Carefully
Your denial letter must include the specific reason for the denial, your appeal rights, and the deadline to file. Find the deadline immediately. Most commercial plans allow 180 days, but some insurers set shorter windows. UnitedHealthcare allows 65 days. Medicare Advantage plans follow CMS guidelines of 60 days. Missing your deadline forfeits your right to appeal.
Step 2: Understand That You Can Appeal Independently
You can file a patient-initiated appeal separate from anything your doctor’s office submits. This isn’t just a backup. Patient appeals carry their own legal protections under the ACA, including mandated response timelines, the right to escalate to an independent external reviewer, and multiple levels of appeal. If your neurologist’s prior authorization was denied, your path is still open.
Step 3: Verify Clinical Details With Your Prescriber
Before building your appeal, confirm with your doctor’s office: Is your migraine frequency clearly documented? Are all prior preventive medication trials listed with specific drugs, dosages, durations, and reasons for discontinuation? Is the correct ICD-10 diagnosis code on file? Was the Emgality prescription written for the correct loading and maintenance dose? If the denial stems from a documentation gap, a corrected PA resubmission may resolve it without a formal appeal.
Step 4: Get a Letter of Medical Necessity
This is the most important document in your appeal. For Emgality, a strong letter of medical necessity from your prescribing neurologist or headache specialist should include your migraine diagnosis and monthly frequency, a detailed history of every prior preventive medication tried (names, doses, duration of each trial, and specific reason each was discontinued, whether for side effects, lack of efficacy, or contraindications), how migraines affect your ability to work, care for your family, and function in daily life, and the clinical rationale for choosing Emgality, including references to the AHS guidelines supporting CGRP therapies as first-line prevention.
How to ask: “My insurance denied Emgality. Would you write a letter of medical necessity for my appeal? I can bring a list of every preventive I’ve tried and what happened with each one.” Specificity wins appeals. Vague statements like “patient failed prior therapies” are far less effective than naming the exact drugs, doses, and outcomes. If your primary care provider submitted the original prescription, consider asking a neurologist or headache specialist to write the appeal letter. Clinicians with specialized headache expertise carry additional weight with insurance medical directors.
Step 5: Build Your Appeal Package
A complete appeal should include a cover letter summarizing your case, the letter of medical necessity from your prescriber, supporting clinical documentation (office notes, headache diary data, treatment history), and a personal statement about how the denial affects your health and life.
The three pillars of a winning appeal:
Your story — How migraines disrupt your daily life. Missed work days, canceled plans, emergency room visits, the toll on your family. This isn’t supplemental. It provides the human weight that clinical data alone can’t communicate.
Clinical evidence — Peer-reviewed studies including the EVOLVE-1 and EVOLVE-2 trial results showing significant reductions in monthly migraine days vs. placebo, the AHS 2024 position statement supporting CGRP therapies as first-line, and any published evidence specific to your situation (the CONQUER trial is especially relevant if you’ve failed multiple prior preventives).
Policy and legal analysis — How your situation meets your plan’s own coverage criteria, applicable state laws, and federal protections under the ACA for appeals and external review.
Step 6: Submit and Track
Follow your denial letter’s submission instructions precisely. Your insurer must respond within 30 days for standard appeals or 72 hours for an expedited appeal (also called an urgent appeal; request this if a delay in treatment could seriously harm your health). Keep records of everything: submission date, method (fax, mail, portal), and all confirmation numbers.
Step 7: Escalate If Needed
If your internal appeal is denied, you have the right to an external review by an independent third party who doesn’t work for your health insurer. External reviewers evaluate medical justification, not the insurer’s financial preferences. These reviews overturn denials more often than most patients expect, because the standard shifts from the insurer’s internal criteria to independent clinical judgment.
The system is designed to wear you down. Persistence is part of the strategy.
An Easier Path: Let Claimable Handle Your Emgality Appeal
If building an appeal from scratch isn’t realistic, or if you’ve already been denied and don’t have the bandwidth for another round, Claimable can handle it for you.
Here’s how it works:
Answer a few questions about your Emgality denial and medical history. We build your case using our database of 4+ million clinical studies, insurer policies, and legal standards. We create a fully customized appeal with your personal story, clinical evidence, and policy analysis. We submit it for you, faxed and mailed directly to your insurer. We guide you through escalation if needed.
Over 80% of Claimable appeals succeed, with most resolved in 10 days or less.
“When my insurance company denied my claim to continue with my medicine, I felt defeated at first… Then I found Claimable. In the end I ended up winning my claim and I couldn’t have done it without Claimable. I highly recommend them.” — April A.
Appealing with Claimable costs $39.95. No success fees, no hidden costs, just a flat fee. When Emgality runs $700 to $970 per month without insurance coverage, the math is straightforward.
Appeal Timelines: How Long Does an Emgality Appeal Take?
| Appeal Stage | Typical Timeline |
|---|---|
| Internal appeal (standard) | Up to 30 days |
| Internal appeal (urgent/expedited) | 72 hours (expedited appeal) |
| External review | 45–60 days |
| Full process (internal + external) | 6–10 weeks |
A complete, well-documented appeal submitted from the start is the fastest path to a decision. The average Claimable appeal gets a response in just 10 days.
FAQs
Why was my Emgality denied if my plan covers it?
Having Emgality on your plan’s formulary doesn’t guarantee automatic approval. Most plans require prior authorization, and those PA criteria typically include step therapy (proof that you’ve tried and failed older preventive medications), minimum migraine frequency thresholds, and specific documentation requirements. Your plan may technically cover Emgality, but “covered” and “approved without a fight” are very different things.
Do I really have to try older medications like topiramate before getting Emgality?
That depends on your insurer’s current policies, but you may not need to start from scratch. If you’ve previously tried and discontinued standard preventatives for any documented medical reason (side effects, intolerances, lack of efficacy, or contraindications) those prior trials should satisfy step therapy requirements. And if your healthcare provider can cite the AHS 2024 position statement recommending CGRP inhibitors as first-line, that strengthens the argument that step therapy shouldn’t apply to your case at all.
Can I appeal an Emgality denial myself, or does my doctor have to do it?
You can appeal yourself. Patient-initiated appeals carry their own legal protections: mandated timelines, the right to external review, and multiple appeal levels. Your appeal is independent of anything your doctor files. Both can proceed simultaneously.
What’s the difference between Emgality and other CGRP injections like Aimovig?
All four injectable CGRP drugs, Emgality, Aimovig (erenumab), Ajovy (fremanezumab), and Vyepti (eptinezumab), are effective preventive therapies for migraines, but they work through slightly different mechanisms. Emgality and Ajovy target the CGRP protein itself (the ligand), while Aimovig blocks the CGRP receptor. Oral CGRP options also exist: Qulipta (atogepant) for prevention and Nurtec (rimegepant) for both prevention and acute treatment. But the injectable monoclonal antibodies offer a different pharmacological approach with once-monthly dosing. The key point: patients who don’t respond adequately to one CGRP medication may respond well to another. Failing on one doesn’t mean the entire class won’t work for you. Your doctor chose Emgality for a reason specific to your clinical situation.
How does the Emgality injection work?
Emgality is a once-monthly injection that you self-administer at home using a prefilled pen or syringe. The first dose is a loading dose of 240mg (two 120mg injections), followed by 120mg once monthly. In clinical trials, patients treated with Emgality experienced approximately 4.7 fewer migraine headache days per month compared to 2.8 fewer days with placebo, with 50% responder rates of approximately 60% over 6 months of treatment. That means about 6 in 10 patients saw their migraine days cut in half or more.
How much does Emgality cost without insurance?
Without insurance or discounts, Emgality costs approximately $700 to $970 per month for the maintenance dose (one 120mg prefilled pen). The first month’s loading dose requires two pens, roughly doubling the initial cost. Eli Lilly offers the Emgality Savings Card for commercially insured patients, which can reduce the monthly cost to as little as $35 (up to $4,900 in annual savings). Patients without commercial insurance may qualify for the Lilly Cares Foundation Patient Assistance Program, which provides Emgality at no cost to qualifying individuals. Note that neither the savings card nor the patient assistance program is available to patients enrolled in Medicare, Medicaid, or other government-funded programs, but Medicaid plans in many states do cover Emgality with copays as low as $4 to $9 per month.
What if my insurer wants me to switch to a different CGRP medication?
If your plan prefers Aimovig, Ajovy, or Vyepti over Emgality, your appeal should explain why your neurologist specifically chose Emgality. Strong grounds for a formulary exception include: you’ve previously tried the preferred alternative without adequate results, the preferred drug is contraindicated for you, or there’s a specific clinical rationale (such as Emgality’s mechanism of targeting the CGRP ligand vs. the receptor). The CONQUER trial demonstrated Emgality’s efficacy specifically in patients who had failed multiple prior preventive categories, evidence that strengthens your case if you’ve been through this before.
Is it worth appealing an Emgality denial?
Yes. The insurance industry relies on patients accepting denials without challenge. Fewer than 1% ever appeal. But denials are frequently the result of incomplete documentation, misapplied criteria, or step therapy requirements that contradict current medical guidelines. Your neurologist prescribed Emgality because your migraines are serious enough to warrant targeted preventive treatment. The appeal is your chance to make that case with the right evidence and legal framework behind you.
Claimable’s physician-led team has helped patients recover millions in care access by fighting insurance denials. We’re SOC 2 Type II certified and HIPAA compliant. Learn more about how Claimable works →
Related: Insurance Denied Ubrelvy? How to Appeal and Get Covered
Featured stories

Download a winning sample appeal
Want to see what it takes to successfully overturn a health insurance denial? Download our sample appeal to learn how we build strong, evidence-based cases that get results.
///////////////////////////////////////////////////////////////////////
//////////////////////////////////////////////////////////////////////////
////////////////////////////////////////////////////////////////////
/////////////////////////////////////////////
Each month, I endure about eight major episodes, each one leaving me exhausted, unable to concentrate, and too unwell to take part in daily life.
The frequency and unpredictability of these symptoms have isolated me socially and limited my capacity to take part in activities most people take for granted.
///////////////////////////////////////////////////////////////////////
//////////////////////////////////////////////////////////////////////////
////////////////////////////////////////////////////////////////////
/////////////////////////////////////////////
Be the first to know
Get the latest updates on new tools, inspiring patient stories, expert appeal tips, and more—delivered to your inbox.
You're on the list!

One of our core principles is to help patients protect their rights and level the playing field with their insurance company. This includes rights to multiple appeals, fair reviews, decision rationale, exceptions when needed, and adequate network access, among others. For more, read our post on patients rights.
For many medications, there's no cost to use Claimable to appeal for qualifying patients – thanks to our network of support partners working to expand access to care.
If you aren't eligible for a no cost appeal, Claimable charges a flat fee of $39.95 + shipping. One simple, straightforward price – no success fees or hidden charges. If appealing with Claimable is unaffordable for you, visit our nonprofit partner Coverage Fund.
Check how much Claimable will cost for your specific situation by starting an appeal and entering your insurance information. So you always know what to expect ahead of time – no surprises.
Claimable’s AI-powered platform analyzes millions of data points from clinical research, appeal precedents, policy details, and your personal medical story to generate a customized appeals in minutes. This personalized approach sets Claimable apart, combining proprietary and public data, advanced analysis and your unique circumstances to deliver fast, affordable, and successful results.
We currently support appeals for over 85 life-changing treatments. Denial reasons may vary from medical necessity to out of network, and we even cover special situation like appealing plans that won’t count your copay assistance towards your deductible (hint: those policies were banned at the federal level in 2023). That said, we are rapidly growing our list of supported conditions, treatments and reasons. You can quickly check eligibility and ask to be notified when your interest becomes available. It helps us know where to focus next 🙂
We think about appeal times in a few ways. First, many professional advocates and experienced patients spend 15, 30 or even 100 hours building an appeal–but with Claimable, this takes minutes. We automate the process of analyzing, researching, strategizing and wordsmithing appeals. Next, there is the process of figuring out where you will send it (hint: expand your reach beyond appeal departments), then printing, mailing and/or faxing your submission. We handle that, too. Finally, there is the time it takes to get a decision. We request urgent reviews when appropriate, and typically receive standard appeal decisions within a couple weeks.
Review periods are mandated by applicable laws, from 72 hours for urgent, 7 days for experimental, 30 days for upcoming and 60 days for received services. Our goal is to get a response as fast as possible, since most of our clients are experiencing long care delays or extreme pain and suffering.
Claims are denied for a variety of reasons, many of which blur definitions. We focus on helping people challenge denials by proving care is needed and meets clinical standards, in addition to addressing specific issues like experimental treatments, network adequacy, formulary or site of care preference exceptions. We don't support denials for administrative errors or missing information, as we think those are best handled by simply resubmitting the claim in partnership with your provider. That said, many of our most rewarding successes have been cases previously though 'unwinnable', with providers and patients who fought tirelessly for months without appropriate response or resolution.
A denial letter is a formal notice from your insurance company explaining why a claim was denied and how you can appeal the decision. Sometimes the notice is included within an Explanation of Benefits. It is a legal requirements; if you didn’t receive one, contact your insurance company.
A letter of medical necessity is a statement from your doctor justifying why a specific treatment is critical to your care and/or urgently needed. You can attach it to your patient appeal to strengthen your case, especially if you are requesting an urgent appeal or need to skip standard ‘step therapy’ requirements. That said, we don’t require them and are often successful without them.
A claim file contains all the documents and communications your health plan used to decide whether to approve or deny your claim. Most health plans are legally required to share this information upon request. According to a ProPublica investigation, reviewing your claim file can help expose mistakes or misconduct by your health plan, which can make your appeal stronger.
Your insurer is required by law to give you written information about how to appeal, including the name of the company that reviewed your claim and where to send your appeal. Your health insurer may work with other companies, such as Pharmacy Benefit Managers (PBMs), Third-Party Administrators (TPAs), or Specialty Pharmacies, to manage your claims. These companies might be responsible for denying your claim and handling the appeal process on behalf of your insurer.
If you don't win your first appeal– don't give up! Many people are successful on their 2nd, 3rd or even 4th try, and future appeals are reviewed by independent entities. That said, we wrote a whole guide to understanding your options, including escalating your appeal and seeking other assistance for covering costs, forgiving debt or even seeking legal or regulatory support.
While both denial rates and appeal success rates vary widely by the type of health plan, state, and insurance company, studies have shown more than 50% of people win their appeal–and we apply strategies to boost your chances of success. Claimable has an 80% appeal success rate. The biggest denial challenge is that most people never appeal–allowing unjust denials to control their healthcare options because they are unaware of their rights or lack the support needed to fight back. No one needs to fight alone–Claimable is here to help. We know first hand that many denials are based on errors, inconsistencies or auto-decisions, and have proven strategies for fighting back against this injustice.
Let’s get you covered.

