Resources

Coverage guides
Your neurologist prescribed Emgality because it’s the right preventive treatment for your migraines. Your health insurer decided otherwise. But an insurance denial isn’t the end of the conversation, and you have legal rights that most patients never exercise.
Emgality (galcanezumab-gnlm) is a calcitonin gene-related peptide (CGRP) monoclonal antibody, one of a class of injectable therapies specifically designed to prevent migraine attacks before they start. Unlike older preventive medications that were originally developed for other conditions and repurposed for migraines, Emgality was built from the ground up to target the CGRP pathway, a biological mechanism central to how migraines work. It received FDA approval in September 2018 for preventive treatment of migraine in adults and is also approved for episodic cluster headache.
Despite strong clinical evidence and more than 90% of commercial health plans including Emgality coverage on their formularies, actually getting that coverage activated is a different story. Most plans require prior authorization, and the majority demand that you try and fail two or more older preventive medications before they’ll approve a CGRP drug like Emgality. If you’re reading this, you’ve likely already hit that wall.
Here’s the reality insurance companies don’t advertise: fewer than 1% of denied claims are ever appealed. When patients do appeal with the right evidence, the results are dramatically different. At Claimable, over 80% of our appeals succeed in established conditions.
This guide explains exactly why Emgality gets denied, what makes these denials often medically unjustifiable, and how to build an appeal that wins, including the clinical arguments, documentation strategies, and legal protections that actually change outcomes.
Our physician-led team has built a database of over 4 million clinical studies, insurer policies, and legal standards to fight denials like yours. We know which arguments overturn Emgality denials, and we know the step therapy tactics insurers use to delay access to CGRP drugs.
Why Insurance Companies Deny Emgality Coverage
Before you do anything else, find the specific reason your insurer denied your prescription. The denial reason determines your entire appeal strategy, and using the wrong argument wastes time you don’t have.
The Step Therapy Problem: Months of Medication Roulette Before You Get What Actually Works
Most Emgality denials come down to one thing: step therapy. Your health insurer requires you to try and fail older, cheaper standard preventatives before they’ll approve a migraine-specific CGRP inhibitor, even when the leading medical society in headache medicine says that requirement is no longer clinically justified.
The medications insurers typically demand you try first weren’t designed for migraines at all. They’re repurposed therapies from other fields: beta-blockers originally developed for blood pressure and heart conditions (propranolol, metoprolol), antidepressants (amitriptyline, venlafaxine), and antiepileptic drugs (topiramate, valproate). Some of these drugs do help some patients, but the side effect profiles are significant, and the dropout rates tell the real story.
Consider topiramate, one of the most commonly required step therapy medications. In clinical trials for migraine prevention, approximately 25% of patients on the standard 100mg dose discontinued treatment due to adverse events. The most common reasons: paresthesia (tingling and numbness), fatigue, and difficulty with concentration and memory. These side effects are severe enough that patients often call topiramate “Dopamax” for its cognitive effects. Beta-blockers can cause fatigue, depression, and exercise intolerance. Antidepressants carry their own constellation of side effects including weight gain, dry mouth, and sedation.
Insurers know all of this. Step therapy isn’t a medical strategy. It’s a cost strategy. The older drugs are cheaper, and the insurer saves money for every month you spend trying medications that may not work and may make you feel worse.
The American Headache Society’s 2024 position statement directly challenges this approach. After reviewing more than a decade of clinical evidence and real-world experience, the AHS now recommends that CGRP inhibitors, including Emgality, should be considered a first-line option for effective migraine prevention, without requiring prior failure of other drug classes. The statement is unequivocal: the cumulative evidence for efficacy, safety, and tolerability of CGRP therapies is significantly greater than that for any established migraine preventive treatment.
When your insurer requires you to spend months cycling through medications with high discontinuation rates and substantial side effects before approving Emgality, they’re overriding the judgment of both your prescribing neurologist and the nation’s leading headache specialists.
The Most Common Emgality Denial Types
| Denial Type | What Your Letter Says | What It Actually Means | Best First Move |
|---|---|---|---|
| Step Therapy Required | “Must try preferred alternatives first” | Insurer wants proof you failed 2+ classes of older preventives | Document prior failures, side effects, or contraindications |
| Not Medically Necessary | “Does not meet medical necessity criteria” | Documentation was insufficient or key details were missing | Resubmit with comprehensive clinical evidence |
| Not on Formulary | “Drug not on preferred drug list” | Plan prefers a different CGRP medication | Request formulary exception with clinical rationale |
| Frequency Threshold Not Met | “Does not meet minimum migraine days” | Insurer says your migraine frequency doesn’t qualify | Document true migraine burden with headache diary |
| Incorrect Diagnosis Code | Varies | Wrong or incomplete ICD-10 code submitted | Work with prescriber to correct coding |
| Prior Authorization Expired | “Authorization no longer active” | Previous PA lapsed and needs renewal | Resubmit with updated treatment response data |
Step Therapy Required
This is the most common reason Emgality injections are denied. Insurers including Aetna, Anthem Blue Cross, Cigna, UnitedHealthcare, Blue Shield, and Humana all typically require documented failure of at least two classes of preventive medications before approving CGRP drugs. The specific requirements vary by plan, but the pattern is consistent: try the cheap options first, even if your doctor has already determined they’re not right for you.
“Failure” is defined more broadly than most patients realize, and that’s where your appeal leverage lives. You don’t need to prove a medication was completely useless. Any of the following counts: the drug didn’t reduce your migraine frequency enough, side effects or intolerances made the drug unbearable, you have a medical condition that contraindicates the drug (cardiovascular disease for beta-blockers, kidney stones for topiramate, pregnancy planning for valproate), or you had to discontinue for any documented medical reason. Prior medication trials from other doctors or previous insurers also count. You shouldn’t have to restart the failure clock every time your coverage changes.
Important: The AHS 2024 position statement specifically states that initiation of CGRP-targeting therapies should not require trial and failure of non-specific migraine preventive medication approaches. This is your strongest clinical argument in any step therapy appeal.
Not Medically Necessary
A medical necessity denial usually means the initial submission didn’t include enough clinical detail, not that your insurer made a careful medical judgment. Common documentation gaps for Emgality include: not specifying the number of migraine days per month, not providing a complete treatment history with specific drug names, dosages, durations, and outcomes, not documenting how migraines impact your ability to work and function, or not explaining why Emgality specifically is the right choice.
For Emgality, your prescriber’s documentation should establish your migraine diagnosis with the correct ICD-10 code, quantify your migraine burden (frequency, severity, and disability), list every prior preventive medication tried with specific reasons each was inadequate, and articulate the clinical rationale for choosing a CGRP monoclonal antibody.
Not on Formulary / Non-Preferred Brand
Some health insurance plans prefer a different injectable CGRP medication, often Aimovig (erenumab), Ajovy (fremanezumab), or Vyepti (eptinezumab), over Emgality. This is typically a pricing decision, not a clinical one. All four injectable CGRP drugs are effective preventive therapies, but they’re not interchangeable for every patient.
This matters for your appeal: Emgality and Ajovy work by binding the CGRP ligand (the protein itself), while Aimovig targets the CGRP receptor. These are meaningfully different mechanisms, and patients who don’t respond to one may respond well to another. If your insurer is asking you to switch to a preferred alternative, and you’ve already tried that medication without adequate results or your neurologist has a specific clinical reason for choosing Emgality, that’s a strong basis for a formulary exception.
The CONQUER trial specifically demonstrated that Emgality is effective in patients who have failed two to four prior preventive medication categories, meaning it has published evidence of working in exactly the population most likely to face insurance barriers.
Frequency Threshold Not Met
Most insurers require a minimum of 4 migraine days per month to qualify for Emgality coverage. If your denial cites this reason, it often means the documentation didn’t clearly establish your migraine frequency, not that you don’t actually meet the threshold. A detailed headache diary showing your true migraine burden, corroborated by your neurologist’s clinical assessment, is typically what’s needed to address this.
Keep in mind that many patients underreport migraine frequency in routine visits. If you experience 4 or more migraine days per month (the standard clinical threshold for considering preventive treatment), make sure that number is explicitly documented in your medical records.
Incorrect Diagnosis Code
Emgality coverage requires specific ICD-10 migraine diagnosis codes. Common codes that support Emgality prescriptions include: migraine without aura (G43.00, G43.01), migraine with aura (G43.10, G43.11), chronic migraine without aura (G43.709, G43.711), and migraine, unspecified (G43.90, G43.91). Using a general headache code like R51.9 (“headache, unspecified”) will almost certainly trigger a denial.
If your denial stems from a coding issue, this is often the simplest fix. Work with your prescriber’s office to verify and correct the submitted diagnosis code.
Prior Authorization Expired
Emgality typically requires reauthorization every 6 to 12 months. If your PA has lapsed, you’ll need to resubmit with updated documentation showing that the medication is still working, ideally including migraine diary data demonstrating continued response (a 50% or greater reduction in monthly migraine days is the standard clinical benchmark). Start the renewal process 30 to 45 days before your current authorization expires to avoid gaps in treatment.
How to Appeal an Emgality Denial: Step by Step
A denial is not a final answer. It’s the beginning of a process that patients are legally entitled to, and that works far more often than the insurance industry would like you to believe.
Step 1: Read Your Denial Letter Carefully
Your denial letter must include the specific reason for the denial, your appeal rights, and the deadline to file. Find the deadline immediately. Most commercial plans allow 180 days, but some insurers set shorter windows. UnitedHealthcare allows 65 days. Medicare Advantage plans follow CMS guidelines of 60 days. Missing your deadline forfeits your right to appeal.
Step 2: Understand That You Can Appeal Independently
You can file a patient-initiated appeal separate from anything your doctor’s office submits. This isn’t just a backup. Patient appeals carry their own legal protections under the ACA, including mandated response timelines, the right to escalate to an independent external reviewer, and multiple levels of appeal. If your neurologist’s prior authorization was denied, your path is still open.
Step 3: Verify Clinical Details With Your Prescriber
Before building your appeal, confirm with your doctor’s office: Is your migraine frequency clearly documented? Are all prior preventive medication trials listed with specific drugs, dosages, durations, and reasons for discontinuation? Is the correct ICD-10 diagnosis code on file? Was the Emgality prescription written for the correct loading and maintenance dose? If the denial stems from a documentation gap, a corrected PA resubmission may resolve it without a formal appeal.
Step 4: Get a Letter of Medical Necessity
This is the most important document in your appeal. For Emgality, a strong letter of medical necessity from your prescribing neurologist or headache specialist should include your migraine diagnosis and monthly frequency, a detailed history of every prior preventive medication tried (names, doses, duration of each trial, and specific reason each was discontinued, whether for side effects, lack of efficacy, or contraindications), how migraines affect your ability to work, care for your family, and function in daily life, and the clinical rationale for choosing Emgality, including references to the AHS guidelines supporting CGRP therapies as first-line prevention.
How to ask: “My insurance denied Emgality. Would you write a letter of medical necessity for my appeal? I can bring a list of every preventive I’ve tried and what happened with each one.” Specificity wins appeals. Vague statements like “patient failed prior therapies” are far less effective than naming the exact drugs, doses, and outcomes. If your primary care provider submitted the original prescription, consider asking a neurologist or headache specialist to write the appeal letter. Clinicians with specialized headache expertise carry additional weight with insurance medical directors.
Step 5: Build Your Appeal Package
A complete appeal should include a cover letter summarizing your case, the letter of medical necessity from your prescriber, supporting clinical documentation (office notes, headache diary data, treatment history), and a personal statement about how the denial affects your health and life.
The three pillars of a winning appeal:
Your story — How migraines disrupt your daily life. Missed work days, canceled plans, emergency room visits, the toll on your family. This isn’t supplemental. It provides the human weight that clinical data alone can’t communicate.
Clinical evidence — Peer-reviewed studies including the EVOLVE-1 and EVOLVE-2 trial results showing significant reductions in monthly migraine days vs. placebo, the AHS 2024 position statement supporting CGRP therapies as first-line, and any published evidence specific to your situation (the CONQUER trial is especially relevant if you’ve failed multiple prior preventives).
Policy and legal analysis — How your situation meets your plan’s own coverage criteria, applicable state laws, and federal protections under the ACA for appeals and external review.
Step 6: Submit and Track
Follow your denial letter’s submission instructions precisely. Your insurer must respond within 30 days for standard appeals or 72 hours for an expedited appeal (also called an urgent appeal; request this if a delay in treatment could seriously harm your health). Keep records of everything: submission date, method (fax, mail, portal), and all confirmation numbers.
Step 7: Escalate If Needed
If your internal appeal is denied, you have the right to an external review by an independent third party who doesn’t work for your health insurer. External reviewers evaluate medical justification, not the insurer’s financial preferences. These reviews overturn denials more often than most patients expect, because the standard shifts from the insurer’s internal criteria to independent clinical judgment.
The system is designed to wear you down. Persistence is part of the strategy.
An Easier Path: Let Claimable Handle Your Emgality Appeal
If building an appeal from scratch isn’t realistic, or if you’ve already been denied and don’t have the bandwidth for another round, Claimable can handle it for you.
Here’s how it works:
Answer a few questions about your Emgality denial and medical history. We build your case using our database of 4+ million clinical studies, insurer policies, and legal standards. We create a fully customized appeal with your personal story, clinical evidence, and policy analysis. We submit it for you, faxed and mailed directly to your insurer. We guide you through escalation if needed.
Over 80% of Claimable appeals succeed, with most resolved in 10 days or less.
“When my insurance company denied my claim to continue with my medicine, I felt defeated at first… Then I found Claimable. In the end I ended up winning my claim and I couldn’t have done it without Claimable. I highly recommend them.” — April A.
Appealing with Claimable costs $39.95. No success fees, no hidden costs, just a flat fee. When Emgality runs $700 to $970 per month without insurance coverage, the math is straightforward.
Appeal Timelines: How Long Does an Emgality Appeal Take?
| Appeal Stage | Typical Timeline |
|---|---|
| Internal appeal (standard) | Up to 30 days |
| Internal appeal (urgent/expedited) | 72 hours (expedited appeal) |
| External review | 45–60 days |
| Full process (internal + external) | 6–10 weeks |
A complete, well-documented appeal submitted from the start is the fastest path to a decision. The average Claimable appeal gets a response in just 10 days.
FAQs
Why was my Emgality denied if my plan covers it?
Having Emgality on your plan’s formulary doesn’t guarantee automatic approval. Most plans require prior authorization, and those PA criteria typically include step therapy (proof that you’ve tried and failed older preventive medications), minimum migraine frequency thresholds, and specific documentation requirements. Your plan may technically cover Emgality, but “covered” and “approved without a fight” are very different things.
Do I really have to try older medications like topiramate before getting Emgality?
That depends on your insurer’s current policies, but you may not need to start from scratch. If you’ve previously tried and discontinued standard preventatives for any documented medical reason (side effects, intolerances, lack of efficacy, or contraindications) those prior trials should satisfy step therapy requirements. And if your healthcare provider can cite the AHS 2024 position statement recommending CGRP inhibitors as first-line, that strengthens the argument that step therapy shouldn’t apply to your case at all.
Can I appeal an Emgality denial myself, or does my doctor have to do it?
You can appeal yourself. Patient-initiated appeals carry their own legal protections: mandated timelines, the right to external review, and multiple appeal levels. Your appeal is independent of anything your doctor files. Both can proceed simultaneously.
What’s the difference between Emgality and other CGRP injections like Aimovig?
All four injectable CGRP drugs, Emgality, Aimovig (erenumab), Ajovy (fremanezumab), and Vyepti (eptinezumab), are effective preventive therapies for migraines, but they work through slightly different mechanisms. Emgality and Ajovy target the CGRP protein itself (the ligand), while Aimovig blocks the CGRP receptor. Oral CGRP options also exist: Qulipta (atogepant) for prevention and Nurtec (rimegepant) for both prevention and acute treatment. But the injectable monoclonal antibodies offer a different pharmacological approach with once-monthly dosing. The key point: patients who don’t respond adequately to one CGRP medication may respond well to another. Failing on one doesn’t mean the entire class won’t work for you. Your doctor chose Emgality for a reason specific to your clinical situation.
How does the Emgality injection work?
Emgality is a once-monthly injection that you self-administer at home using a prefilled pen or syringe. The first dose is a loading dose of 240mg (two 120mg injections), followed by 120mg once monthly. In clinical trials, patients treated with Emgality experienced approximately 4.7 fewer migraine headache days per month compared to 2.8 fewer days with placebo, with 50% responder rates of approximately 60% over 6 months of treatment. That means about 6 in 10 patients saw their migraine days cut in half or more.
How much does Emgality cost without insurance?
Without insurance or discounts, Emgality costs approximately $700 to $970 per month for the maintenance dose (one 120mg prefilled pen). The first month’s loading dose requires two pens, roughly doubling the initial cost. Eli Lilly offers the Emgality Savings Card for commercially insured patients, which can reduce the monthly cost to as little as $35 (up to $4,900 in annual savings). Patients without commercial insurance may qualify for the Lilly Cares Foundation Patient Assistance Program, which provides Emgality at no cost to qualifying individuals. Note that neither the savings card nor the patient assistance program is available to patients enrolled in Medicare, Medicaid, or other government-funded programs, but Medicaid plans in many states do cover Emgality with copays as low as $4 to $9 per month.
What if my insurer wants me to switch to a different CGRP medication?
If your plan prefers Aimovig, Ajovy, or Vyepti over Emgality, your appeal should explain why your neurologist specifically chose Emgality. Strong grounds for a formulary exception include: you’ve previously tried the preferred alternative without adequate results, the preferred drug is contraindicated for you, or there’s a specific clinical rationale (such as Emgality’s mechanism of targeting the CGRP ligand vs. the receptor). The CONQUER trial demonstrated Emgality’s efficacy specifically in patients who had failed multiple prior preventive categories, evidence that strengthens your case if you’ve been through this before.
Is it worth appealing an Emgality denial?
Yes. The insurance industry relies on patients accepting denials without challenge. Fewer than 1% ever appeal. But denials are frequently the result of incomplete documentation, misapplied criteria, or step therapy requirements that contradict current medical guidelines. Your neurologist prescribed Emgality because your migraines are serious enough to warrant targeted preventive treatment. The appeal is your chance to make that case with the right evidence and legal framework behind you.
Claimable’s physician-led team has helped patients recover millions in care access by fighting insurance denials. We’re SOC 2 Type II certified and HIPAA compliant. Learn more about how Claimable works →
Related: Insurance Denied Ubrelvy? How to Appeal and Get Covered
Your doctor prescribed Nurtec ODT because it's the right treatment for your migraines. Your insurer said no. But you don't have to just give up on Nurtec. If it's the right treatment for you, let's talk about how to get covered.
Nurtec ODT is the only oral CGRP medication approved by the FDA for both treating acute migraines and preventing them. That dual role is a genuine clinical advantage, and it's precisely what makes the insurance process so frustrating. Insurers may apply different criteria depending on whether your doctor prescribed Nurtec for acute use, preventive use, or both, and many patients (and even some prescribers) don't realize the way the prescription is written directly determines which criteria the insurer evaluates.
Here's what Pfizer's own data says: 97% of patients with commercial insurance have plans that cover Nurtec ODT. If you were denied, that means that there's likely a path to getting covered through an appeal — whether it's through demonstrating that you meet the criteria, updating paperwork, or proving you deserve an exception to their rules.
If you're denied Nurtec, you can appeal
Fewer than 1% of denied claims are ever appealed. Insurance companies count on that. But when patients do appeal with the right evidence, they often win. At Claimable, we see this in practice — with over 80% of our appeals getting approved in established conditions.
This guide walks you through exactly why your Nurtec coverage was denied, how to identify your specific denial type, and what a winning appeal actually looks like, including the timelines, documentation, and strategies that work.
Why Insurance Companies Deny Nurtec Coverage
Understanding the specific reason for your denial is the single most important step before doing anything else. The denial reason determines your entire strategy, and getting it wrong means wasting time on arguments that won't work for your situation.
What Makes Nurtec Denials Uniquely Complicated
Most migraine medications do one thing: treat an attack or prevent future ones. Nurtec does both. That's a significant clinical advantage, but it creates a coverage problem that doesn't exist with drugs like Ubrelvy (acute only) or Qulipta (prevention only).
If your doctor prescribed Nurtec for acute use, the insurer applies one set of criteria, typically requiring you to have tried and failed triptans first. If prescribed for prevention (every-other-day dosing), the insurer applies a different, often stricter set of criteria — requiring documented failure of older preventive drugs like beta-blockers, antidepressants, or antiepileptics.
If your doctor intended Nurtec to serve both roles, the prior authorization may need to address both sets of requirements simultaneously. Many prescribers don't realize this, and many PAs are submitted addressing only one indication.
The quantity of tablets prescribed can also trigger a denial. Preventive dosing requires roughly 15 tablets per month, while acute use calls for up to 8. A prescription for 15 tablets submitted with acute-only documentation will get flagged immediately.
The mismatch between how the prescription is written and what the insurer's criteria require is one of the most common, and most preventable, reasons Nurtec gets denied.
The Most Common Types of Nurtec Denials
Most articles list denial types using the language insurers put in their letters. We think about denial types based on what they actually mean for patients and how they shape your strategy.
Step Therapy Required
This is the most common Nurtec denial. Insurers require patients to try and fail older medications first — especially triptans — before approving Nurtec, even when your doctor has clinical reasons for prescribing it first.
For acute use, most plans require documented failure of two or more triptans (sumatriptan, rizatriptan, zolmitriptan, eletriptan). For preventive use, the bar is even higher — many plans require failure of medications from two or more drug classes: beta-blockers (propranolol, metoprolol), antidepressants (amitriptyline, venlafaxine), antiepileptics (topiramate, valproate), or other CGRP therapies.
What most patients don't realize: "Failure" doesn't mean the drug didn't work. Side effects, contraindications, and medical reasons a drug is inappropriate also count as failure. For example, many patients with cardiovascular disease can't safely take triptans, which means insurers should not require them to try these medications first.
Important: The American Headache Society's 2024 position statement explicitly recommends CGRP-targeting therapies — including Nurtec — as a first-line option for migraine prevention, without requiring prior failure of older drug classes. When an insurer demands you fail on beta-blockers or topiramate before accessing Nurtec, they're contradicting the leading medical society's guidance. That's a powerful argument in any appeal.
Not Medically Necessary
This denial often means the initial submission was too thin, not that your insurer reviewed your full history and determined Nurtec isn't appropriate. Common gaps: not specifying migraine frequency, not listing comorbidities, not documenting impact on daily functioning, or not explaining why Nurtec specifically is the right choice.
A Nurtec watch-out: Because the drug is approved for both acute and preventive use, the prescriber needs to clearly document which indication is being requested and why. A submission that doesn't specify this can trigger a medical necessity denial even when you need it.
Quantity Limit Exceeded
Many insurers set a default quantity limit of 8 tablets per month, aligned with acute use. If your doctor prescribed Nurtec for prevention (roughly 15 tablets per month), the prescription may automatically get flagged.
This is often a straightforward fix: your prescriber submits documentation confirming the preventive indication and requests a quantity override. But the quantity limit PA criteria are often separate from the initial coverage PA, so you may need to clear two hurdles, not one.
Not on Formulary / Non-Preferred Brand
Some plans prefer a different CGRP medication — often Ubrelvy for acute use, or Qulipta, Aimovig, Emgality, or Ajovy for prevention. This isn't a medical judgment about whether you need the medication, it's a business decision about which drugs the insurer has negotiated pricing for.
The strongest argument centers on Nurtec's dual indication. If your doctor prescribed it for both acute treatment and prevention — which no other oral CGRP medication can do — replacing it with two separate drugs increases complexity, cost, and adherence burden. That's a compelling case for a formulary exception.
PA Requirements Not Met
This denial means the insurer believes one or more coverage criteria weren't satisfied. In many cases, the issue isn't that you actually fail the criteria — it's that the insurer applied the rules incorrectly, ignored clinical details, or relied on outdated requirements.
Common scenarios: migraine frequency disputes (your documented frequency meets the threshold but wasn't clearly presented), indication mismatch (the PA was submitted for one indication but the quantity suggests another), or incomplete treatment history (the documentation didn't fully capture your prior medication trials).
Incorrect Diagnosis Code
Coverage often hinges on submitting the correct ICD-10 diagnosis code. Common issues include using a general headache code instead of a specific migraine code, or failing to specify episodic migraine when requesting preventive coverage. Pfizer's own resources flag incorrect codes as one of the most common reasons for Nurtec PA denials. This is often the easiest denial to fix.
A breakdown of common ICD-10 diagnosis codes for migraine treatment:
Duplicate CGRP Therapy Denial
If you're already taking an injectable CGRP (Aimovig, Ajovy, or Emgality) for prevention, some insurers will deny Nurtec for acute use, claiming you can't use two CGRP drugs at the same time. This denial is often wrong — the American Headache Society and published clinical evidence support using a CGRP monoclonal antibody for prevention alongside an oral gepant for acute treatment, because they work through different mechanisms. Overturning this typically requires a detailed clinical rationale from a neurologist or headache specialist.
How to Appeal a Nurtec Denial: Step by Step
Appeals work far more often than most people think. The insurance industry has spent decades conditioning patients to accept "no" as final. It's not.
Step 1: Read Your Denial Letter Carefully
Your denial letter is required by law to include the specific reason for denial, your appeal rights, and the deadline to file.
Find your deadline. Most commercial plans allow 180 days, but deadlines vary significantly by insurer. UnitedHealthcare gives you just 65 days for most plan types — less than half the time Aetna, BCBS, and Cigna allow. Medicare Advantage plans follow CMS guidelines of 60 days. Missing the deadline means you won't be allowed to appeal, so move as quickly as possible.
Step 2: Understand That You Can Appeal, Not Just Your Doctor
You can file an appeal yourself, as the patient, separate from (or in addition to) your doctor filing a provider-level appeal. Patient-initiated appeals often have stronger legal protections than provider appeals — including mandated response timelines, the right to escalate to an independent external reviewer, and multiple levels of appeal. If your doctor's prior authorization or appeal was denied, that doesn't mean yours will be. They're different processes.
Step 3: Clarify the Prescription With Your Doctor
Before gathering documentation, confirm with your prescriber: Was Nurtec prescribed for acute treatment, preventive treatment, or both? Was the PA submitted with the correct indication and quantity? Were the correct ICD-10 migraine codes used?
If the issue is a mismatch between the prescription and the PA submission, a corrected resubmission may resolve the denial without a formal appeal.
Step 4: Get a Letter of Medical Necessity
A letter of medical necessity (LOMN) from your prescribing physician is the single most important document in a Nurtec appeal. It should include documentation of your migraine days per month, prior medication history and diagnosis code.
How to ask your doctor: Be direct. "My insurance denied Nurtec. Would you be willing to write a letter of medical necessity for my appeal? I can bring information on what the insurer typically looks for." Some doctors aren't experienced with writing these, but offering a template or outline can help significantly.
Step 5: Build Your Appeal Package
Your appeal should include a cover letter summarizing your case, the letter of medical necessity from your doctor, supporting clinical documentation (records showing migraine frequency, treatment history, comorbidities), and a personal statement explaining how the denial affects your health and daily life.
The three pillars of a winning appeal:
- Your story — the personal health impact of this denial
- Clinical evidence — studies, guidelines, and medical records supporting Nurtec for your situation
- Policy and legal analysis — how your situation meets coverage criteria under your plan, state law, and federal regulations
Step 6: Submit and Track
Submit your appeal per the instructions in your denial letter. Your insurer is required to respond within 30 days for standard appeals, or 72 hours for urgent/expedited cases. Keep records of when you submitted, how (fax, mail, portal), and any confirmation numbers.
Step 7: Escalate If Needed
If your internal appeal is denied, you have the right to an external review by an independent third party not employed by the insurer. External reviews commonly overturn denials that make it to that stage — because the reviewer evaluates whether the denial was medically justified, not whether the insurer wants to pay.
Don't give up after one "no." The system is designed to make you quit. Persistence is part of the strategy.
An Easier Path: Let Claimable Handle Your Nurtec Appeal
If navigating this process feels overwhelming, or if you just don't have time to become an expert in insurance appeals, Claimable can help.
Here's how it works:
- Answer a few questions about your Nurtec denial and medical history
- We build your case using our database of 4+ million clinical studies, insurer policies, and legal standards
- We create a fully customized appeal with your personal story + clinical evidence + policy analysis
- We submit it for you, faxed and mailed directly to your insurer
- We guide you through escalation if needed
80%+ of Claimable appeals succeed, with most resolved in 10 days or less.
"When my insurance company denied my claim to continue with my medicine, I felt defeated at first... Then I found Claimable. In the end I ended up winning my claim and I couldn't have done it without Claimable. I highly recommend them." — April A.
Appealing with Claimable is just $39.95. No success fees, no hidden costs. Just a simple flat fee. If your migraine medication costs $1,000+ per month, the math is simple.
Appeal Timelines: How Long Does a Nurtec Appeal Take?
The faster you submit a complete, well-documented appeal, the faster you'll get a decision. While these timelines seem slow, getting your appeal right can speed things up significantly. The average Claimable appeal gets a response in just 10 days.
FAQs
Why was my Nurtec denied if my plan covers it? Having Nurtec on your plan's formulary doesn't mean it's automatically approved. Most plans require prior authorization, and the PA criteria often include step therapy requirements, quantity limits, or documentation thresholds that aren't obvious from your benefits summary. Pfizer reports that 97% of commercial plans cover Nurtec — but "covered" and "approved without a fight" are very different things.
Can I appeal a Nurtec denial myself, or does my doctor have to do it? You can appeal yourself. Patient-initiated appeals often have stronger legal protections than provider appeals, including mandated timelines and the right to external review. You can appeal in addition to your doctor's appeal — they're separate processes.
What if my insurer wants me to try Ubrelvy instead of Nurtec? This is a step therapy requirement. Your appeal should focus on why Nurtec specifically is the right choice. If you need both acute and preventive coverage, Nurtec is the only oral gepant approved for both — that's a strong clinical argument against switching to a drug that only covers one indication.
How many tablets should I be prescribed? For acute use, up to 8 tablets per month. For prevention, approximately 15 tablets per month (75 mg every other day). The maximum is 18 doses in a 30-day period. If your doctor prescribed preventive dosing, make sure the PA was submitted for the preventive indication.
Can I take Nurtec with an injectable CGRP medication like Aimovig? Some insurers will deny this combination, but clinical evidence and AHS guidance support using a CGRP monoclonal antibody for prevention alongside an oral gepant for acute treatment. If you receive a duplicate therapy denial, a detailed clinical rationale from your neurologist is essential.
What's the difference between Nurtec and other CGRP medications? CGRP medications aren't interchangeable. Nurtec is the only oral gepant approved for both acute treatment and prevention of episodic migraine. Ubrelvy and Zavzpret are acute-only. Qulipta is prevention-only. Aimovig, Ajovy, Emgality, and Vyepti are injectable monoclonal antibodies for prevention.
How much does Nurtec cost without insurance? Approximately $1,000+ for an 8-tablet dose pack. Pfizer offers a savings card for commercially insured patients that can reduce the cost to as little as $0/month (with a $7,000 annual cap), and a first-fill program providing one prescription at no cost while benefits are verified.
Is it worth appealing? Yes. The insurance industry counts on patients giving up — fewer than 1% of denials are ever appealed. But when patients do appeal with proper documentation, overturn rates are significant. You've already been prescribed this medication by a doctor who believes you need it. The appeal is your chance to make that case.
Claimable's physician-led team has helped patients recover millions in care access by fighting insurance denials. We're SOC 2 Type II certified and HIPAA compliant. Learn more about how Claimable works →
Related: Why Was My Migraine Treatment Denied? Common Insurance Denial Reasons and How to Fight Back
Some insurance plans do cover Zepbound for sleep apnea, but coverage almost always requires prior authorization and the right documentation from your provider. If your plan denies the request, that denial is worth appealing, especially since Zepbound is the only GLP-1 medication with FDA approval specifically for obstructive sleep apnea.
The coverage landscape is shifting fast. CVS Caremark dropped Zepbound from its formulary entirely in mid-2025. Multiple class-action lawsuits have been filed challenging these denials. And Medicare now has a specific pathway for Zepbound coverage when prescribed for obstructive sleep apnea (OSA), with a government agreement expected to cap the copay cost at roughly $50/month starting in 2026.
Whether you're trying to figure out if your plan will cover Zepbound before you fill the prescription at your pharmacy, or you've already been denied and need to know what to do next, this guide walks through coverage requirements by plan type, the most common denial reasons, and exactly how to build an appeal that addresses each one.
Does Insurance Cover Zepbound for Sleep Apnea?
Sometimes, yes, but it's usually not automatic.
Coverage generally depends on whether Zepbound is on your plan's formulary, whether you meet your plan's prior authorization requirements, and whether the correct documentation is submitted with the initial request.
Here's why the OSA indication matters so much: Zepbound (tirzepatide) is a GIP/GLP-1 polypeptide receptor agonist and the only GLP-1 medicine FDA-approved to treat moderate-to-severe obstructive sleep apnea in adults with obesity. That means even if your plan limits coverage of GLP-1s for weight loss, you may still have a path to get Zepbound covered for sleep apnea. This distinction is the foundation of most successful appeals.
What Insurers Typically Require for Coverage
This varies by plan, but the most common things insurance wants to see are below. Call your insurer or visit your member website for a full list of coverage criteria. You can see example coverage criteria from CVS Caremark here.
The CVS Caremark Situation
CVS Caremark removed Zepbound from most formularies effective July 1, 2025, after striking a rebate deal with Wegovy's manufacturer Novo Nordisk. Patients have been directed to switch to Wegovy instead.
For OSA patients, this creates a particularly strong basis for a formulary exception: Wegovy is not FDA-approved for sleep apnea. Zepbound is the only GLP-1 with that indication, so there is no formulary alternative with the same FDA-approved use.
As plans renew for 2026, many patients are receiving similar notifications that Zepbound will not be covered in the new year.
Multiple ERISA class-action lawsuits have been filed challenging CVS Caremark's denials.
Medicare Coverage for Zepbound and Sleep Apnea
Medicare Part D may cover Zepbound when prescribed specifically for moderate-to-severe OSA in adults with obesity. This is because Medicare does not cover Zepbound for weight loss alone (federal law excludes anti-obesity medications from Part D unless they have another FDA-approved indication). The December 2024 OSA approval created the coverage pathway that didn't exist before.
CMS proposed expanding Part D to include anti-obesity medications for 2026, but the government decided against it, which means the OSA indication remains the only Medicare pathway for Zepbound.
Key details for Medicare plans:
- Coverage depends on whether your specific Part D plan has added Zepbound for OSA to its formulary. Check using the Medicare.gov Plan Finder or call the number on your card.
- Starting as early as April 2026, a government agreement with Eli Lilly is expected to cap the Medicare copay at approximately $50/month.
- The 2026 annual out-of-pocket costs for Part D is $2,100.
- Medicare Advantage plans (Part C) vary; some have added Zepbound for OSA, others haven't.
- Prior authorization is almost always required.
- Lilly savings cards are not available to government-insured patients (Medicare, Medicaid, Tricare).
If your Part D plan denies coverage, Medicare has its own escalation path: redetermination within 120 days, then QIC reconsideration, then ALJ hearing.
Common Denial Reasons and What to Do About Each One
When it comes to Zepbound for sleep apnea, all of the common denial reasons can be challenged. It's about identifying the right steps to take. Look for language like these in your denial letter under "why your request was denied."
Need help figuring out which reason applies to you and what strategy to use? Use Claimable's guided appeals tool to make it easy.
Prior Authorization Incomplete / Missing Documentation
What it looks like: "Insufficient information," "missing documentation," "clinical records not provided."
What to do: Contact your prescriber's office to find out exactly what was submitted. Compare it against your plan's requirements, then resubmit with a complete packet: sleep study, BMI documentation, diagnosis notes, and treatment plan.
"Not Medically Necessary"
What it looks like: "Does not meet criteria," "not medically necessary."
What to do: Get a copy of your plan's coverage criteria and compare it against your records point by point. File an appeal that directly addresses each criterion, and include a letter of medical necessity from your healthcare provider. If your insurer's criteria don't align with FDA labeling or clinical guidelines, flag that in the appeal.
Not on Formulary
What it looks like: "Not covered," "non-formulary," "preferred alternatives required."
What to do: Appeal and request a formulary exception. Since Zepbound is the only GLP-1 approved for sleep apnea, your exception request has a strong foundation. If the plan is suggesting Wegovy or another GLP-1, those drugs are not FDA-approved for OSA. Clearly state why the suggested alternatives are not appropriate for your diagnosis.
Plan Exclusion / "Weight Loss Only"
What it looks like: "Plan excludes weight-loss medications," "not a covered benefit."
What to do: This is a mis-categorization issue. Zepbound prescribed for OSA is a treatment for a sleep disorder, not a weight-loss prescription. Confirm with your provider that the PA was submitted under ICD-10 code G47.33 (OSA), not obesity. If the coding was correct and the denial still cites a weight-loss exclusion, appeal and clearly distinguish between the two indications.
Step Therapy / Alternative Required
What it looks like: "Must try X first," "step edit."
What to do: If you've already tried alternatives (CPAP, other medications, lifestyle interventions) and they didn't adequately manage your OSA, document those attempts in your appeal. Note that no other GLP-1 is FDA-approved for OSA. Also, 37+ states have step therapy protection laws that may limit your insurer's ability to enforce these requirements.
How to Appeal a Zepbound Sleep Apnea Denial
Most people will be able to reverse a Zepbound denial for sleep apnea when they appeal with the right argument, documentation, and clinical backing. Here's the high-level process.
Your appeal should mirror the denial reason. Quote the denial reason directly, respond with the specific evidence that addresses it, and attach supporting documents with the relevant sections highlighted. Key documents include your denial letter, sleep study report, OSA diagnosis/severity, BMI documentation, provider notes, and (recommended) a letter of medical necessity from your prescribing provider.
Important deadline: Most commercial plans give you 180 days from the denial date to submit an internal appeal. Don't miss it.
If your first appeal is denied, you can request a second-level internal appeal. After exhausting internal appeals, most plans are required by law to offer access to external review through an independent organization. Your final denial letter should include instructions on how to request it.
Read our full guide to appealing a Zepbound denial for a detailed, step-by-step walkthrough of the appeals process.
How to Get Ahead of a Denial Before It Happens
If your doctor is considering prescribing Zepbound for sleep apnea, you can get ahead of coverage issues from the start.
What to ask your insurer (call the number on your insurance card):
- Is Zepbound covered for obstructive sleep apnea under my specific plan?
- Is it on formulary? If not, what's the exception process?
- What are the prior authorization criteria, and where is the PA form?
- Where should the PA be submitted (portal/fax)?
- What are typical timelines, and what qualifies for an expedited review?
What to confirm with your provider before the PA is submitted:
- Sleep study report and AHI documentation are attached
- Current BMI/weight documentation is included
- Diagnosis is coded under OSA (G47.33), not obesity
- Clinical rationale ties directly to the plan's stated criteria
- Submission goes to the correct portal or fax number
Ongoing Legal Challenges to Zepbound OSA Denials
Several lawsuits are now challenging insurers' categorical denials of Zepbound for sleep apnea. A class-action suit filed in September 2025 alleges CVS Caremark and CareFirst BlueCross BlueShield wrongfully denied coverage in violation of ERISA. A separate suit in New York challenges CVS Caremark's blanket formulary removal. And a third targets Elevance (Anthem) for denying OSA coverage while covering other GLP-1s for different conditions.
These cases are still in progress, but they signal that many denials may not be consistent with plan terms or federal law. Learn more about the legal landscape here.
How Claimable Helps
Navigating insurance appeals is time-consuming and confusing, especially when you're dealing with a condition that affects your sleep and daily functioning. Claimable's appeals tool helps you:
- Identify the most likely reason behind your denial
- Build a customized appeal letter backed by clinical evidence, policy analysis, and relevant legal protections
- Automatically mail and fax your appeal to the right place
- Escalate to the next level if your first appeal is denied
Start your Zepbound sleep apnea appeal with Claimable →
FAQs
Does insurance cover Zepbound for sleep apnea? Some plans do, but coverage typically requires prior authorization. Your provider will need to submit documentation including your sleep study, OSA diagnosis, and BMI. If your plan denies coverage, you have the right to appeal.
What do I do if insurance denies Zepbound for sleep apnea? Get your denial letter and identify the specific reason. Common reasons include missing documentation, "not medically necessary," formulary exclusion, benefit exclusion, or step therapy requirements. File an appeal that directly addresses the stated denial reason with supporting evidence.
Does Medicare cover Zepbound for sleep apnea? Medicare Part D may cover Zepbound when prescribed for moderate-to-severe OSA in adults with obesity. Medicare does not cover it for weight loss alone. A government agreement is expected to cap the Medicare copay at approximately $50/month starting as early as April 2026.
Does CVS Caremark cover Zepbound? As of July 2025, CVS Caremark removed Zepbound from its standard formulary. However, since Zepbound is the only GLP-1 FDA-approved for OSA, you may have strong grounds for a formulary exception.
Can I appeal a plan exclusion denial for Zepbound for sleep apnea? In many cases, yes. Most benefit exclusions apply to weight-loss medications. Since Zepbound is FDA-approved for OSA, a prescription for sleep apnea should not fall under a weight-loss exclusion. Appeal and clearly distinguish between the OSA and weight-loss indications.
What is a formulary exception? A formulary exception is a request for coverage of a medication that isn't on your plan's list of covered drugs. For Zepbound and OSA, the exception argument is particularly strong since no other GLP-1 has FDA approval for sleep apnea.
How long do I have to file an appeal? Most commercial plans give you 180 days. Medicare patients have 120 days. Check your denial letter for exact deadlines.
What clinical evidence supports Zepbound for sleep apnea? The SURMOUNT-OSA trials showed Zepbound reduced breathing disruptions by 55-63% over 52 weeks. Up to 51.5% of participants no longer met OSA criteria after one year.
Insights & updates
Dr. Warris Bokhari, Co-Founder and CEO of Claimable, was named to the 2026 TIME100 Health List of the World's Most Influential Leaders in Health. The annual list celebrates innovators and pioneers working to build healthier populations around the world.
The recognition is truly meaningful. And for those of us building alongside Warris, it reflects something we've seen up close for years — steady advocacy, rigorous thinking, and a deep commitment to standing up for patients when it matters most.
We wanted to take a moment to share more about the person behind the recognition and the principles that guide his work.
A path shaped by lived experience
Warris’s work has always been personal.
He was raised in England by two parents living with long-term disabilities. His mother lived with severe rheumatoid arthritis, and his father retired when Warris was still a child because of chronic back problems. Affordable, guaranteed access to healthcare wasn’t an abstract concept in their household — it was a daily reality, directly influencing stability, opportunity, and quality of life.
That experience stayed with him. Warris trained and practiced as a physician in the UK before moving to the United States, where he later held leadership roles across major healthcare and technology organizations, including GE Healthcare, Amazon, Apple, and Anthem.
Over time, he developed a clear-eyed view of how modern U.S. healthcare actually functions — not as a system optimized for care, but as one structured around financial risk, complexity, and friction — a stark contrast to the system he experienced growing up in the U.K.
Again and again, he saw the same outcome: patients prescribed necessary care, only to face delays or denials driven more by financial incentives than medical judgment.
Why Claimable exists
Claimable was born from that inequity. Warris didn’t set out to build a healthcare company. He set out to address an escalating crisis and change what happens when patient care collides with a system built around cost control.
He brought together co-founders Alicia Graham and Zach Veigulis around a clear conviction: patients deserve real support in those moments — not more paperwork, not more waiting, and not a process designed to wear them down. From the beginning, Claimable has been built on a simple principle: patients shouldn’t have to become experts, advocates, or adversaries just to access care.
For Warris, that means not only building tools that support patients at scale, but stepping in personally when the stakes demand it.
The cases people never see
Some of the most meaningful advocacy Warris does happens out of view, supporting patients in situations where access to care is genuinely life-or-death. This includes complex organ transplant denials and advanced oncology cases, where clinical nuance, timing, and judgment matter deeply.
In many of these cases, Warris has taken the lead, navigating the medical complexity and policy reasoning that ultimately shape critical coverage decisions. Being directly involved in these moments has been both sobering and instructive, reinforcing how much responsibility comes with building in this space.
That hands-on engagement doesn’t just shape his perspective — it informs our research and development efforts, pioneering strategies in new conditions and therapies before translating them into tools within Claimable. It has pushed the boundaries of what we believe can be done at scale by combining clinical rigor with purpose-built technology. And it continually sharpens our understanding of what good judgment looks like under pressure.
“I’ve worked closely with Warris on some of the most difficult cases we’ve encountered. What stands out is his steadiness — knowing when to push, when to pause, and how to carry the weight of decisions that affect real lives.” — Zach Veigulis, Co-Founder & CAIO, Claimable
Real Patient Impact
Take the story of Keaton, a 35-year-old father who was diagnosed with Stage IV bile duct cancer confined to his liver. After an extensive multidisciplinary review, he had been fully cleared for a transplant at Houston Methodist. Despite being his only potentially curative option, the transplant was denied, effectively forcing Keaton toward palliative care.
His wife, Tori, posted online asking for help, and Warris didn’t hesitate. He stepped into one of the most complex and visible cases imaginable, not because it was easy, but because it was right.
Warris immersed himself in the clinical research, the transplant criteria, and the insurer’s policy language — and just as importantly, in Keaton’s story. He got to know the family. He understood what was on the line.
Keaton later wrote, “I honestly might not be alive today if it weren’t for Warris and the team. They are highly knowledgeable and genuinely want to help people. I would recommend them to anyone and everyone if you’re having issues with insurance or being denied a life-saving treatment like I was.”
Keaton’s story isn’t unique in Warris’s world. It’s representative of the calls he answers every day — quietly, urgently, and when the outcome matters most.
Advocate first, CEO second
Warris has always led as an advocate first: for patients, for providers, and for the integrity of medicine itself. Inside the company, that philosophy becomes culture.
He stays closely connected to the lived reality of navigating denials and keeps the urgency of this mission front and center. Whether cold-calling early provider partners, supporting families facing devastating denials, or digging into emerging research on new therapies, he sets the tone for how we operate.
Leading by example, Warris encourages us to be bold in our convictions, resourceful in our approaches, and unwavering in our integrity. That mindset has led to clear non-negotiables for Claimable: the patient story must be central; evidence must be expert-curated and accurate; patients’ rights must be defended, not sidelined; and there must always be a next step.
“I’m honored to work alongside Warris, who is a doctor by training and by creed — someone who takes ‘do no harm’ seriously in every interaction. He reminds all of us that this work is about more than overturning denials. It’s about restoring trust.” — Alicia Graham, Co-Founder & COO, Claimable
Warris’s recognition on the TIME100 Health list reflects years of difficult, often invisible work, and reinforces why Claimable exists in the first place. The lessons learned alongside individual patients continue to shape how we build — embedding empathy, rigor, and real-world insight into tools designed to support patients at scale. We’re incredibly proud of Warris for this well-deserved recognition. And we’re even more committed to the journey ahead.

On July 1, CVS Caremark began forcing patients to switch from Zepbound to Wegovy – and we quickly took action to help folks fight back by appealing. With many patients protected by step therapy and non-medical switching laws, we were confident in their cases. The majority of these denials should have been overturned easily.
They weren't.
Our team quickly started noticing an unusual – and troubling – pattern. Appeals were getting denied at a high rate and at unusual speed. Denials were coming back not in the standard hours or days, but in minutes – all following the same script and formula, returned with almost identical responses. Same wording. Same rationale. Same disregard for the patient's actual medical needs.
Under federal law, every appeal is supposed to get a full, fair, individualized review by a human reviewer. These weren't reviews. They were copy-paste auto-replies. This falls well outside of what we've been used to from insurers, and it raised serious legal concerns.
Seeing the patterns in the data
The appeals process is typically fragmented, with individual patients and providers rarely compiling or comparing notes. Spotting trends is nearly impossible. But by handling hundreds of appeals specifically for CVS's Zepbound forced-switch patients, Claimable had a unique vantage point. We saw systemic, policy-wide denials unfolding in real time. These weren't a few isolated cases; we were seeing a consistent, repeated pattern of patients being denied their legal rights.
We immediately began supporting second-level appeals and escalation to independent review, including a detailed opinion from our Senior Legal Advisor, D. Brian Hufford, Esq., of The Hufford Law Firm PLLC, to help patients fight for the coverage they deserved. More appeals began to succeed – but not nearly enough.
Our success rate doubled after escalating cases with stronger legal arguments, but it remained below our usual benchmarks. That wasn't good enough. We knew something was deeply wrong. So even while individual appeals were starting to work, it was clear that this broader pattern of systemic denials raised bigger legal questions – questions that went beyond what the appeals process alone can fix.
So with Brian, we began investigating additional options.
The CVS Caremark Zepbound lawsuit and your right to a full, fair, individualized review
Working closely with patients we'd supported through their appeals, Brian took the evidence to Berger Montague, a firm that specializes in healthcare class action litigation.
On September 3, 2025, they filed a class action lawsuit against CVS Caremark on behalf of patients in ERISA-governed employer-sponsored health plans whose coverage for Zepbound was denied and whose appeals were rejected based on medical necessity.
The lawsuit alleges that CVS Caremark wrongfully denied coverage by issuing denials that appeared to rely on templated language, despite patients meeting the plans' criteria for medical necessity. Filed under ERISA, the suit alleges that CVS Caremark:
- Breached its fiduciary duties by prioritizing financial gain over medical appropriateness or plan obligations;
- Engaged in prohibited transactions by entering formulary agreements that benefit its own bottom line;
- Violated the terms of employer health plans by denying coverage for an FDA-approved, medically necessary treatment – while steering patients toward non-equivalent or off-label alternatives; and
- Ignored federal claims procedure standards by failing to provide timely, transparent, and individualized appeal reviews.
The complaint asks the court to issue injunctive relief, requiring CVS to change its policies going forward. It also seeks other appropriate equitable relief if those remedies are found insufficient to fully address the harm to patients.
Advocacy doesn't end with the appeal
Since July 1st, we've helped hundreds of patients file appeals for Zepbound denials. That's only a tiny slice of the hundreds of thousands of patients affected. But it's enough to spot the trend and push for accountability.
To be clear: Claimable isn't a party to this suit. The relief it seeks isn't on our behalf. But for us, being a patient-first company means taking a root cause approach to solving problems whenever possible. In this case, it meant going beyond the appeals process we operate within and connecting patients to legal options they might not otherwise access.
We built Claimable to make appealing easier and more successful. But just as importantly, we built it to expose what's really happening behind the scenes. Denials don't happen in isolation, and neither can our response.
That's why we're proud to support a broader movement for change, alongside legal teams, advocacy organizations, and policy leaders. Appeals are one piece. Litigation is another. Legislative reform is critical too. The only way to deter unjust denials is to challenge them—again and again—until insurers and pharmacy benefit managers face real consequences for saying no without cause.
What's next for Zepbound appeals
Legal action takes time, and we'll be watching closely as this case makes its way through the courts. But while the system may be slow, we're not slowing down. We will continue helping patients appeal these Zepbound forced switches – and we'll keep evolving our strategies as new evidence and appeal precedents emerge.
We hope this lawsuit sends a clear message: insurer misconduct that puts patients at risk will not go unnoticed or unchallenged.
Our job isn't just to make paperwork easier and arguments stronger. It's to fight back when something feels wrong. To listen to patients. To advocate. To act.
And we won't stop until everyone gets the care they need and coverage they deserve.
At Claimable, we’re dedicated to empowering patients to fight for the care that they deserve. That’s why, as of today, we’re officially supporting free second-level appeals for CVS Caremark Zepbound forced-switch denials — so you can be confident your case receives a full, fair, and individualized review.
First, What’s A Second-Level Appeal?
When you submit an appeal as a patient and it’s denied, it isn’t the end. You have the right to request a second-level appeal, which often involves review by a different department or an independent third party. Put simply? It’s another chance to have your case heard, and have your denial overturned.
Why We’re Escalating to Second-Level Appeals
Over the past weeks, we’ve had an influx of patients file appeals for Zepbound coverage with CVS Caremark. Unfortunately, we’ve begun to see responses to those appeals come back as form-letter denials – ignoring not only your unique health history, doctor’s notes, and plan details, but also state and federal laws. Federal rules are clear: every appeal must receive an individualized review. The copy paste answers we’re seeing? They’re not that.
In order to make sure that each of these appeals get the full and fair review they’re entitled to, it’s time to escalate it to the next level:
- Internal vs. External Reviews
- Internal appeal: Your denial is reviewed by CVS Caremark or your insurer. Yes, the same company that issued the denial – though federal law requires that the review be conducted by someone who wasn’t involved in the original decision.
- External appeal: Also called an external review or, in some states, an Independent Medical Review (IMR). This is conducted by a licensed medical professional or organization not affiliated with your insurance provider, using objective, evidence-based criteria. External decisions are binding on the insurer, but you may still have the right to pursue legal action if the outcome is unfavorable.
For forced-switch denials of Zepbound, we pursue the external review – most likely to secure the coverage you need — free of charge.
What to Expect If Your First Zepbound Appeal Is Denied
- You Report the Denial
Once you get the notification that your appeal has been denied, simply log into your Claimable account to report the outcome – or email us at support@getclaimable.com - You Consent To Escalation
We’ll confirm you’d like to continue to escalate to a second-level appeal. At this point, you’ll upload your appeal denial letter. - We Build Your Strongest Case
Once you consent, we’ll generate your second-level appeal package. This includes a newly drafted appeal letter with an expert legal opinion and your prior appeal materials. - You Review & Submit
We’ll notify you when your second-level appeal is ready for review. You’ll confirm where to send (fax/mail) your appeal, then click “Submit” once everything looks right. - We Send – Expedited
Claimable will fax and mail your appeal to both CVS and the independent reviewer.
Because all Zepbound forced-switch appeals involve ongoing treatment for a serious condition, your case will be marked urgent – requesting an expedited external review. This means that in most cases, the reviewer must issue a decision within 72 hours, though some may take longer.- You Get Notified
You’ll be notified of the outcome via portal message, email, or phone, as well as receiving a mailed copy of the decision.
If it’s approved? The decision is binding – and CVS must cover your Zepbound.
Key Questions – Answered
What is a second-level appeal?
It’s your right to request another review when your first appeal is denied—either internally by the insurer or externally by an independent reviewer. We choose the path most likely to win for you.
Why is Claimable offering free 2nd-level appeals?
With these early Zepbound appeals, we’ve seen a clear pattern of “cookie-cutter” denials that violate the full-fair-and-individualized-review requirement. To level the playing field, we’re offering these escalations free of charge to demand unbiased consideration.
Keep in mind, this only applies if you submitted your first-level appeal through Claimable. If you've appealed a different way and think you might need a second-level appeal, feel free to email us for help navigating the process.
What’s included in my Claimable second-level appeal?
A freshly drafted appeal letter with expert legal commentary, your first appeal materials, and previous denial letters—packaged to maximize your chance of success.
Is there any cost to second level appeals?
Nope – this service is completely free for CVS Caremark Zepbound forced-switch cases. Claimable’s appeal strategy is customized for each insurer and medication—and in these cases, supporting a second-level appeal is part of our core approach to winning.
What do I need to submit a second-level appeal?
You’ll need your appeal denial letter to confirm the instructions for submitting a second-level appeal, including where to send it and whether any forms are required.
If you’ve received your claim file and designated record set since initially submitting, we recommend uploading them when prompted (after you review your second-level appeal draft).
How do I track my appeal’s status?
If you haven’t heard back within 72 hours, call the number on your insurance card. Otherwise, we’ll notify you as soon as the reviewer issues a decision.
Do I have to redo the appeal questionnaire?
Never. All your first-level answers and uploads carry over automatically.
We know the appeals process can feel confusing and overwhelming. That’s why we built Claimable — to guide you every step of the way. With our new second-level appeal support, you can rest assured that we’ll fight tirelessly to get you the coverage you deserve.
Questions? We’re here for you. Reach out to support anytime.
Appeal education

Mounjaro is the only dual GIP/GLP-1 available for type 2 diabetes, and your doctor prescribed it for a reason. When your insurer sends back a denial, it can feel like the end of the conversation. It isn’t.
Most commercial insurance plans and Medicare Part D formularies cover Mounjaro for type 2 diabetes, but “covered” doesn’t always mean to it's accessible. Prior authorization requirements, step therapy that tries to push you onto older medications first, and formulary restrictions (usually driven by rebate deals rather than clinical data) all create barriers between you and the prescription your doctor wrote. And if Mounjaro was prescribed off-label for weight loss, coverage can be an uphill battle. Because it's so complicated, many patients give up on treatment entirely after a denial rather than navigate the appeals process.
Less than 1% of denied claims get appealed, so the insurance industry assumes you’ll just accept their decision. That assumption saves insurers billions every year. But the low appeal rate says more about how opaque the process is than how unlikely you are to win. Patients who do push back with solid evidence see dramatically higher overturn rates. At Claimable, our appeals succeed over 80% of the time in established conditions.
The type of denial you received matters a lot in terms of how to write your appeal. A formulary restriction is different from a step therapy requirement, and this guide walks you through how to respond to each.
Why Insurance Companies Deny Mounjaro Coverage
Before building your appeal, find the specific reason that your insurance denied coverage. Understanding your denial type means that you can fight it with the correct arguments.
What We See Across Thousands of GLP-1 Appeals
Denial letters use insurer language that's designed to sound final, even though most denials are anything but. Here’s how to decode the most common denial types for Mounjaro, what they actually say about your situation, and where to begin:
Off-Label Use Denials: The Weight Loss Problem
Mounjaro is FDA-approved only for type 2 diabetes. It isn't approved for weight loss, while Zepbound is – even though both contain tirzepatide. If Mounjaro is prescribed to a patient for weight loss, most insurers will deny coverage. That denial is hard to overturn because it’s technically correct.
Your options: If you have type 2 diabetes, the problem may be a coding issue rather than a real coverage dispute (see Step 0 below). If you don’t have diabetes and are seeking tirzepatide for weight management, consider asking your doctor about Zepbound, the version of tirzepatide that carries an FDA-approved weight management indication. If your prescriber believes off-label Mounjaro is clinically appropriate for a specific comorbidity, some plans will consider a formulary exception with a strong letter of medical necessity (though this is a harder fight).
Step Therapy Denials
Step therapy means that you have to fail cheaper medications before the insurer will approve Mounjaro. That usually means metformin first, and sometimes a second-line oral agent like a sulfonylurea, DPP-4 inhibitor, or SGLT2 inhibitor. Some plans also require failure of a single-mechanism GLP-1 like semaglutide before approving a dual-mechanism one like Mounjaro.
The detail most patients miss: “failure” has a broad medical definition that works in your favor. Intolerable side effects, contraindications based on your medical history (even if you never took a dose), and inadequate glycemic control all qualify. If alternatives are clinically inappropriate, your doctor can request a step therapy exception. The SURPASS-2 trial, which demonstrated Mounjaro’s superiority over semaglutide at every dose, provides strong clinical rationale for why a “try semaglutide first” requirement may not serve your best interest.
Not Medically Necessary Denials
This denial rarely reflects a thorough clinical review. It usually means the PA submission lacked documentation, and it’s one of the most commonly overturned denial types on appeal.
What a strong submission requires: your current A1C, documented diabetes management history, comorbidities, prior medications tried and their outcomes, relevant lab work, and a clear rationale for why Mounjaro’s dual GIP/GLP-1 mechanism is clinically appropriate for your situation. If your initial submission was thin, a resubmission with thorough documentation can change the outcome entirely.
Not on Formulary / Non-Preferred Denials
This is more common with Mounjaro than with older GLP-1s. Many plans drug lists prefer semaglutide products because of pricing negotiations, regardless of the head-to-head clinical data that favors tirzepatide.
How to respond: Request a formulary exception. Every insurer is required to have one for non-formulary drugs that are medically necessary. Your case is strongest if formulary alternatives have failed, caused side effects, or are contraindicated. If you’ve already been responding well on Mounjaro, continuity of care is a powerful argument.
PA Requirements Not Met
This means the insurer says you didn’t satisfy one or more specific criteria, such as an A1C threshold, documented metformin use, or comorbidity documentation. Insurers sometimes misapply their own rules or overlook submitted documentation. Review each criterion against your records and address gaps directly in your appeal.
Quantity Limit Denials
If your prescriber wrote for a dose or quantity that exceeds your plan’s default limits, your prescriber should submit a quantity or dose override request with documentation showing why the prescribed amount is medically appropriate.
How to Appeal a Mounjaro Denial: Step by Step
The initial denial is a starting point, not a verdict. Appeals exist because first-pass coverage decisions get it wrong all the time.
Step 0: Confirm Your Prescription is Coded Correctly
Before launching a formal appeal, rule out a coding error. A surprising number of Mounjaro denials trace back to a mismatch between the diagnosis code on the prescription and the drug’s FDA-approved indication.
If your prescriber submitted a vague code instead of a specific type 2 diabetes code (E11 and its subcategories), or if the prescription was flagged as weight management, the claim may have been auto-rejected without anyone reviewing your clinical history.
Getting the code corrected and resubmitting the prior authorization can resolve the issue.
Step 1: Read Your Denial Letter Carefully
Your denial letter is required by law to include the specific reason for denial, your appeal rights, and the deadline to file.
Find your deadline first. Most commercial plans allow 180 days, but there are important exceptions: UnitedHealthcare allows just 65 days for many plan types, and Medicare Advantage plans follow CMS guidelines of 60 days. Missing the deadline eliminates your right to appeal entirely.
Step 2: Understand That You Have Your Own Appeal Rights
Your provider can appeal on the clinical side. But you also have the right to file your own appeal as the patient, and it runs on a separate track with its own legal protections.
Why this matters: Patient-initiated appeals carry guaranteed response timelines, external review rights, and multiple appeal levels that provider-level appeals may not offer.
Use both tracks: Your doctor makes the clinical case while you exercise your independent rights. If your prescriber’s prior authorization was denied, that doesn’t close the door on your side of the process.
Step 3: Get a Letter of Medical Necessity
A letter of medical necessity (LOMN) from your prescribing physician is an important document in your appeal package.
What a strong LOMN for Mounjaro should include: your diagnosis codes (E11.x for type 2 diabetes, plus relevant comorbidity codes), current and historical A1C levels, documented comorbidities, a summary of prior treatments tried and why each was insufficient or inappropriate, supporting clinical evidence from the SURPASS trials (particularly SURPASS-2 if the insurer is pushing a semaglutide alternative), and a clear explanation of why Mounjaro’s dual GIP/GLP-1 mechanism is the clinically appropriate choice for your situation.
How to ask: Be direct with your doctor. “My insurance denied Mounjaro. Would you be willing to write a letter of medical necessity for my appeal? I can provide information on what the insurer typically looks for.” If your doctor’s office hasn’t written many of these, offering to share a template can improve the quality and completeness of the letter. You can download our LOMN template here and forward it to your provider.
Step 4: Build Your Appeal Package
Your submission should include a cover letter summarizing your case, the letter of medical necessity, supporting clinical documentation (A1C history, lab results, visit notes, weight and metabolic data), and a personal statement explaining how the denial has affected your health and daily life.
A winning appeal weaves together three elements:
Your story: The real-world impact of being denied this medication, and how it affects your ability to manage your health, work, and daily life. The person reviewing your appeal is a human being, and personal context shifts how they read the clinical data.
Clinical evidence: A1C reductions of up to 2.07% in SURPASS-1, superiority over semaglutide across all doses in SURPASS-2, and up to 92% of participants reaching the ADA’s target A1C using the efficacy estimand. Tailor the evidence to your specific clinical situation.
Policy and legal analysis: How your case satisfies your plan’s own coverage criteria, applicable state insurance laws, and federal protections under the ACA. If the denial contradicts the insurer’s published medical policy, name the contradiction explicitly.
Step 5: Submit and Track
Submit to your insurer per the instructions in your denial letter. They’re required to respond within 30 days for standard appeals (72 hours for urgent appeals).
Keep records: Save confirmation numbers, note submission dates and methods (fax, mail, portal), and write down the name of every person you speak with. Documents go missing in insurer systems more often than you’d expect, and a clear paper trail is your best protection.
Step 6: Escalate If Needed
If your internal appeal is denied, that’s still not the end. You have the right to an external review conducted by an independent third party with no ties to the insurer. External reviewers assess the clinical evidence on its own terms, not through the lens of the insurer’s cost structure, and they overturn internal denials regularly.
State Department of Insurance complaints and ERISA-specific remedies for employer-sponsored plans are additional escalation paths.
Don’t give up after one “no.” The entire system is built around the assumption that you’ll stop after the first rejection. Be persistent.
Mounjaro’s FDA-Approved Indications: Why They Matter for Your Appeal
Mounjaro’s clinical profile is narrower than some other GLP-1s in terms of FDA-approved indications, but its efficacy data within those indications is among the strongest available.
Type 2 diabetes in adults (approved May 2022): As the first and only dual GIP/GLP-1 receptor agonist, Mounjaro was approved based on the SURPASS trial program. SURPASS-1 demonstrated A1C reductions of up to 2.07% as monotherapy. SURPASS-2 showed superiority over semaglutide 1 mg at all three doses. Using the efficacy estimand, A1C reductions reached up to 2.46% versus 1.86% for semaglutide, and up to 92% of participants reached the ADA’s target A1C of less than 7%. Using the treatment-regimen estimand, A1C reductions reached up to 2.30% versus 1.86%, with up to 86% reaching target.
Type 2 diabetes in pediatric patients (approved December 2025): Expanded to include patients 10 years of age and older with type 2 diabetes inadequately controlled with metformin, basal insulin, or both. The pediatric indication covers the 5 mg and 10 mg doses only, based on the SURPASS-PEDS trial results; the 15 mg dose was not studied in pediatric patients.
Unlike Ozempic, Mounjaro does not currently carry separate FDA-approved indications for cardiovascular risk reduction or chronic kidney disease. This means appeals that rely on cardiovascular or renal arguments need to reference the clinical literature rather than an on-label indication. That said, Mounjaro’s superior head-to-head data against semaglutide for glycemic control remains a powerful differentiator when insurers try to substitute a less effective alternative.
How Long Does a Mounjaro Appeal Take?
Complete submissions help your appeal move faster. In some cases, Claimable submits appeals to both internal and external review simultaneously to compress the timeline.
The Easier Path: Let Claimable Handle Your Appeal
If you’d rather not navigate this process alone, Claimable can help.
Here’s how it works: You provide a few details about your denial and medical history, and we generate a fully customized appeal backed by our work across millions of clinical studies, insurer policies, and legal standards. We fax and mail it for you, so no trips to the post office or hassle to print.
We’ve handled thousands of GLP-1 cases, so we know which arguments work with which insurers, what to escalate and when, and we’re here to help you through any questions you may have.
Appealing with Claimable costs $39.95 (plus shipping) for a Mounjaro appeal, with no success fees or hidden charges. When the medication itself runs over $1,000 a month without coverage, that’s a small price to keep a treatment that’s working.
FAQs
Can I file my own appeal, or does my doctor handle that? Both. Your provider appeals on the clinical side, but you have a separate right to appeal as the patient, with its own legal protections and mandated response timelines. Running both tracks simultaneously gives you the best chance of getting the denial reversed. See Step 2 above.
What’s the difference between Mounjaro and Zepbound? Same molecule (tirzepatide), different FDA approvals. Mounjaro is approved for type 2 diabetes management. Zepbound is approved for chronic weight management and obstructive sleep apnea. If you are seeking tirzepatide for weight management and don’t have type 2 diabetes, Zepbound is the labeled product. Insurance coverage comes down to which diagnosis code is submitted.
Does Medicare cover Mounjaro? Medicare Part D covers Mounjaro for type 2 diabetes, though prior authorization is typically required. The Inflation Reduction Act’s $2,100 annual out-of-pocket cap for 2026 provides meaningful cost protection. Medicare does not cover Mounjaro for weight loss.
My insurer wants me to try a different GLP-1 first. What’s the argument against that? SURPASS-2 directly compared tirzepatide to semaglutide and found tirzepatide delivered superior A1C reductions at every dose. If your insurer is requiring you to try semaglutide before approving Mounjaro, that step therapy requirement asks you to use a medication that performed less effectively in the head-to-head data. Your prescriber can cite SURPASS-2 in a step therapy exception request.
How much does Mounjaro cost without insurance? The list price is approximately $1,080 per month. If you have commercial insurance and a type 2 diabetes diagnosis, the Mounjaro Savings Card can reduce your copay to as little as $25 per month, or up to roughly $499 per month if your commercial plan doesn’t cover the medication. For self-pay patients, Mounjaro is now available through LillyDirect at around $299 per month for any dose. Government insurance beneficiaries (Medicare, Medicaid, TRICARE) are not eligible for the savings card but may qualify for assistance through the Lilly Cares Foundation.
Is it worth appealing? Almost always. The insurance industry’s denial system is calibrated around the fact that virtually nobody challenges them. When patients do file appeals with complete documentation, the results are far better than the initial denial would suggest. Your doctor prescribed Mounjaro for a reason, and an appeal forces someone to evaluate that clinical reasoning on its merits rather than rejecting it on a technicality.
Claimable has recovered over $30 million in care value for patients. Our platform is SOC 2 Type II certified and HIPAA compliant, and our appeals are reviewed by licensed physicians. Learn more about how we work →
Getting denied coverage for Humira is stressful enough on its own. If you live with a chronic condition like rheumatoid arthritis, Crohn’s disease, or psoriasis, a denial can feel like a direct threat to your health, especially if you’re already on the medication and staring down a gap in treatment.
If you're reading this, you've already done the most important thing: you know you can appeal, and you're looking for the tools to do it well. A template is a smart place to start. The thing worth knowing is that a template alone isn't usually what wins and appeal. Insurers review thousands of appeal letters, and a generic one that says "my doctor recommends Humira" without specific clinical evidence is easy to deny. The letter that gets approved is the one you tailor with the right details, and that's exactly what this guide is built to help you do.
This guide shows you how to file your own Humira appeal with a letter built to get approved, not just submitted. We’ll walk through the template section by section, explain how to tailor your approach to your specific insurance type, and cover what to do if your first appeal comes back denied.
If you’d rather not navigate this alone, Claimable builds fully customized appeal letters using a purpose-built database of clinical studies, insurer policies, and laws, then mails and faxes them directly to your insurer.
Why Humira Denials Are So Common Right Now
For nearly two decades, Humira had almost no competition. That changed fast. The first adalimumab biosimilar, Amjevita, launched in January 2023, and a wave of others followed that summer, including Cyltezo, Hadlima, and Hyrimoz. With lower-cost alternatives suddenly on the market, pharmacy benefit managers moved quickly to steer their formularies toward biosimilars and away from brand-name Humira.
The most consequential move came from CVS Caremark, one of the largest PBMs in the country, which removed Humira from its major national commercial formularies effective April 1, 2024. Other large PBMs have made similar changes for subsequent plan years. The result is a surge of denials that simply didn’t exist a few years ago, hitting two very different groups of patients: people who are newly prescribed Humira and being told to try a biosimilar first, and people who have been stable on Humira for years and are now being pushed to switch.
Both situations are appealable. The right argument just depends on which denial you’re facing.
The Most Common Reasons for Humira Denials
Before you write a single sentence, find the exact reason your insurer denied coverage. It’s printed on your denial letter, and it determines your entire strategy. Submitting the wrong type of response wastes time and can burn through your limited appeal opportunities.
If your denial came down to something fixable, like missing lab work or screening results that your plan requires before approving Humira, you may not need a full appeal at all. A corrected resubmission with the missing documents attached can sometimes resolve it faster. Our guide to Humira denials breaks down how to match each denial type to the right response.
Humira Appeal Letter: What to Include, Plus a Customizable Template
We’ve put together a free, customizable appeal letter template you can use to appeal your Humira denial. You can download a copy here:
Download the free appeal letter template
Before you download it, here’s an overview of everything a strong Humira appeal should include, and why each section carries the weight it does.
Section 1: Your Information, Their Information, and Claim Details
The letter opens with a header block identifying you, your insurer’s appeals department, and the specific claim being appealed. Follow it with an opening paragraph that names the medication, your prescribing physician, your diagnosis, and the insurer’s stated reason for denial, copied word for word from the denial letter. Matching their exact language matters, because your job in the rest of the letter is to dismantle that specific reason.
If a gap in treatment would harm your health, this is also where you request an expedited review. Many plans are required to decide expedited appeals far faster than standard ones, often within 72 hours.
Section 2: Diagnosis and How It Affects Your Life
Here you lay out your diagnosis, including the ICD-10 code if you have it, any comorbidities, and a specific description of your symptoms and how they affect your daily life. This is the part of the letter that makes the human cost of the denial concrete. A reviewer who reads that you’ve missed work, lost mobility, or can’t care for your family reads the rest of your argument differently.
Section 3: Prior Treatments Tried and Failed
This is where you prove you’ve already satisfied step therapy and prior authorization requirements. Document every medication and treatment you tried before Humira in a simple table:
Specific dates, drug names, and outcomes are what turn “I’ve tried other things” into documented evidence the insurer has to reckon with. If you’re being forced off Humira and onto a biosimilar, this section is also where you note that you were stable on Humira and that switching carries real clinical risk for you.
Section 4: Why This Medication Is Medically Necessary
This section ties together your physician’s recommendation, your clinical profile, and any improvement you’ve already seen on Humira (or expect to see if you haven’t started yet). It should also spell out what happens without it: disease progression, irreversible joint or organ damage, hospitalization risk, or loss of function. Medical necessity is the standard most denials hinge on, so this is where you meet it head-on.
Section 5: Clinical Evidence Supporting This Treatment
This is the most research-intensive section, and the one that separates a strong appeal from a hopeful one. Cite specific clinical studies, professional society guidelines, and the FDA labeling that support Humira for your condition. Name the trials, quantify the outcomes, and connect each piece of evidence directly to the insurer’s stated reason for denial.
One serious warning: never cite a study you haven’t verified. Fabricated or misquoted clinical references do more damage than no citation at all. A reviewer who catches one invented study has every reason to distrust your entire letter. We’ll come back to this, because it’s the single biggest risk in the era of AI-generated appeals.
Section 6: Your Denial Doesn’t Align With Your Insurer’s Own Policies
Insurers publish their coverage criteria for Humira, and those documents are public. Pull your plan’s policy, find the criteria, and demonstrate point by point that you already meet them. There is nothing more persuasive than showing that a denial contradicts the insurer’s own written rules. This is also one of the places where insurers count on patients not looking, because the process is built to be opaque.
Section 7: Applicable State and Federal Law
Citing the law transforms your appeal from a personal request into a legal demand, and insurers handle those very differently. The protections available to you depend on your state and the type of plan you have, but they often include step therapy override laws, prior authorization response-time requirements, ERISA protections for employer plans, ACA guarantees of internal and external appeal rights, and your right to an independent external review.
Step therapy override laws are worth understanding in particular. Most states now have them, and they commonly bar a plan from making you repeat step therapy you’ve already completed, including under a previous insurer, and they often require the plan to accept your prescriber’s attestation that a required drug failed as evidence of that failure. If you’ve already tried and failed the biosimilar your plan is now demanding, that’s not just a clinical argument. In many states, it’s a legal one. Our formulary exception guide covers how to invoke these protections when your drug has been excluded.
Section 8: Request for Review and Approval
Close with a clear, formal request: approve coverage for Humira, override the specific barrier cited in the denial, and, if your treatment is time-sensitive, process the appeal on an expedited basis. Ask for written confirmation of the decision, and if the appeal is denied, request a complete copy of your claim file so you can see exactly what the reviewer considered.
Section 9: Supporting Documentation Enclosed
List everything you’re attaching: your physician’s letter of medical necessity, relevant medical records, the clinical studies you cited, any prior appeal decisions, and lab results. A reviewer should never have to go looking for the evidence that backs your argument.
Section 10: Citations and References
End with a references section listing every study, guideline, insurer policy, and law you cited, formatted so a reviewer can locate each source. This is also your own final check: if you can’t produce a clean citation for a claim, that claim shouldn’t be in the letter.
An Alternative Approach: Use Claimable
The template above gives you the structure of a strong appeal. But the sections that carry the most weight, namely the clinical evidence, the insurer policy analysis, and the legal citations, are also the ones that take hours of research and carry real risk if you get them wrong. A fabricated study or a misapplied law can sink an appeal that would otherwise have won.
Claimable was built to solve exactly this problem. You answer a set of straightforward questions about your denial, diagnosis, and treatment history, and Claimable generates a fully personalized appeal letter drawing on a purpose-built database of clinical studies, insurer policies, and laws. Every citation is verified. Every argument is tailored to your specific insurer and plan type. We’ll even mail and fax it to your insurer for you.
More than 80% of Claimable appeals succeed, with most resolved in 10 days or less, delivering industry-leading results.
Start your appeal with Claimable.
Common Mistakes That Get Humira Appeals Denied
Missing or Incomplete Documentation
The most common reason appeals fail has nothing to do with the strength of the argument. It’s missing paperwork. Patients submit lab results that are too old to satisfy the plan’s screening requirements, forget to include the original denial letter, or list prior medications without the specific dates and dosages that make them count as evidence. Before you send anything, make sure every claim in your letter is backed by a document in the envelope.
Using Vague or Generic Language
“The patient needs this medication” tells a reviewer nothing. Vague appeals fail because they don’t engage with the actual reason for denial and don’t give the reviewer anything specific to approve. The fix is specificity: name your disease activity scores, your failed treatments and why they failed, and the exact clinical reason Humira is right for you. Emotion belongs in your letter, but it supports the evidence rather than standing in for it. Lead with the clinical case and let the personal impact reinforce it.
Missing the Deadline
Deadlines are unforgiving, and missing one can cost you your appeal rights entirely. Under the ACA, plans generally must give you at least 180 days from the date of your denial to file an internal appeal, and 4 months after a final internal denial to request an external review. But the specifics vary by plan type and state. ERISA employer plans, Medicare, and Medicaid each run on their own timelines, and some are considerably shorter. Expedited appeals have tighter windows still. The safest move is to mark your calendar the day your denial arrives and file as early as you can, while your documentation is freshest. Your exact deadline is printed on your denial letter.
Citing Inaccurate Information
This is the fastest-growing way to lose an appeal, and it’s worth dwelling on. General-purpose AI tools and generic template letters can often produce fabricated clinical studies and incorrect legal citations that look completely real. If your appeal references a study that doesn’t exist or a law that doesn’t say what you claim, it doesn’t just fail to help. It damages your credibility and gives the reviewer a clean reason to deny. So, always verify every clinical study and legal reference before it goes anywhere near your insurer.
This is also exactly why Claimable was built differently. Claimable’s proprietary AI runs on a purpose-built database of real clinical studies, real laws, and real policy data, not a general-purpose chatbot guessing at citations. Every appeal is checked before it goes out. Start your appeal.
What to Do If Your First Appeal Is Denied
A first denial is not the end of the road. It’s the first step on a path that has several more, and patients who keep going win far more often than patients who stop. Here’s the full map.
Level 1: Internal Appeal
Your first appeal goes back to the insurer, where it must be reviewed by someone who wasn’t involved in the original decision. Treat a second internal appeal as a chance to strengthen your case rather than simply resubmit it. Address every specific deficiency the insurer cited, add any new clinical evidence or updated records you can gather, and shore up your physician’s letter of medical necessity if the first one was thin. It’s also worth asking your doctor to request a peer-to-peer review, where they speak directly with the insurer’s medical director. For specialty medication denials, these conversations have a strong track record of overturning the original decision.
Level 2: External Review
Once you’ve exhausted internal appeals, you can request an independent external review, where a reviewer who doesn’t work for your insurer evaluates your case. This is one of the most powerful rights you have, and one of the least used. In most plan types, the external reviewer’s decision is binding, meaning the insurer must comply if the denial is overturned. Many states run their own external review processes with their own timelines and procedures, so check the rules where you live.
Level 3: Regulatory Complaints and Other Options
If you’ve worked through internal and external review and still need leverage, you have more options. For state-regulated plans, filing a complaint with your state’s Department of Insurance can add real pressure, and many states have patient advocacy offices or managed care ombudsman programs that can help. For high-value or especially complex cases, a consultation with an attorney who handles insurance disputes may be worthwhile. The system is designed to wear people down. Knowing that these escalation paths exist is often what keeps a winnable appeal alive.
Frequently Asked Questions
How long do I have to appeal a Humira denial?
Under the ACA, plans generally must give you at least 180 days from your denial to file an internal appeal, and 4 months after a final internal denial to request an external review. ERISA employer plans, Medicare, and Medicaid run on their own timelines, some shorter, so always check the deadline printed on your denial letter.
Can I appeal if my insurer dropped Humira from its formulary?
Yes. A formulary exclusion is appealable through a formulary exception request, in which you argue that the covered alternatives are inappropriate for you, often because you’ve already tried and failed a biosimilar or were stable on Humira before the switch was forced. Your plan’s own coverage criteria and applicable step therapy laws are central to this argument.
Do I need my doctor to file the appeal?
No. You have the right to file your own appeal, and patient appeals carry legal protections that provider appeals don’t, including mandated response timelines and external review rights. Your doctor’s letter of medical necessity strengthens your case, and a patient appeal and a provider appeal filed together create pressure from two directions.
What’s the difference between Humira and a biosimilar, and does it matter for my appeal?
Biosimilars are highly similar to Humira and approved to treat many of the same conditions, but “similar” isn’t “identical.” Some patients experience differences in side effects, injection devices, or how well their condition stays controlled. If you’ve had a documented problem on a biosimilar, that experience is important evidence in an appeal to stay on or return to Humira.
Will citing clinical studies and laws really make a difference?
Yes, as long as they’re accurate. Specific clinical evidence and applicable law are what move an appeal from a personal request to a documented, legally grounded demand. Just be certain every citation is real and correctly stated, because a single fabricated reference can sink an otherwise strong appeal.
Don’t Appeal Alone If You Don’t Have To
You have the right to appeal, the law is often on your side, and Humira denials are overturned every day by patients who know how to build their case. The template above gives you the structure to do it yourself.
If you’d rather not spend hours researching studies and verifying legal citations, Claimable handles the hardest parts for you, builds an appeal tailored to your insurer and plan, and submits it on your behalf. More than 80% of our appeals succeed, with most resolved in 10 days or less.
You're right to ask this question. After years of data breaches making headlines, apps harvesting personal information for advertising, and AI tools with murky privacy policies, being cautious about where your health data goes is smart. It's exactly what you should be doing.
So here's the straightforward answer: yes, your health data is safe with Claimable. But you shouldn't just take our word for it – that’s why we’ve brought in independent 3rd parties to evaluate and certify every piece of our operations. Here's what those certifications mean, what protections are actually in place, and how to think about the services you choose to trust with your information.
What counts as protected health information,and where it lives today
Any time you interact with the healthcare system, you generate what's legally known as protected health information, or PHI. That includes your diagnoses, prescriptions, lab results, treatment history, insurance details, and billing records. PHI is created every time you see a doctor, fill a prescription, file an insurance claim, use a patient portal, or receive lab results.
The organizations that handle this information — your physician's office, pharmacy, insurance company, lab, telehealth platform — are all governed by the same core federal law: HIPAA, the Health Insurance Portability and Accountability Act. HIPAA exists specifically to ensure that any entity handling your health data meets strict standards for how it's stored, transmitted, and accessed.
Claimable handles PHI in the course of building your appeal, and we’re fully HIPAA certified. That means we’re held to the same standards as your doctor's office or your insurance company.
What HIPAA compliance actually means
HIPAA gets referenced constantly in healthcare, but most people have never had someone explain what it actually requires in practical terms.
At its core, HIPAA sets rules for how organizations that handle PHI must store, transmit, and control access to that data. It covers things like who within an organization can see your records, how data must be encrypted so it can't be intercepted, what happens in the event of a breach, and under what circumstances your information can be shared with anyone else.
HIPAA isn't a one-time checkbox. It's an ongoing set of requirements that covered organizations must maintain, document, and be able to demonstrate compliance with at any time.
Claimable completed a third-party HIPAA attestation through cybersecurity firm Workstreet in November 2025. That means an independent organization reviewed our data handling practices, security controls, and policies against HIPAA requirements and confirmed that we meet them. This is a higher bar than self-attestation — it means someone from outside the company verified it.
Any partner that handles protected health information on Claimable's behalf is also covered by a Business Associate Agreement (BAA), which legally requires them to maintain the same HIPAA standards.
The security side: What SOC 2 Type II means, in plain English
If HIPAA is the healthcare-specific standard, SOC 2 Type II is the gold standard for security in the technology industry — the way companies prove their systems are trustworthy to the organizations and people who depend on them.
Here's the simplest way to think about it: an independent auditing firm comes in and examines how a company protects data — not just on paper, but in practice, over an extended period of time. They look at security controls, access management, encryption, monitoring, incident response, and operational processes. Then they either certify the company or they don't.
The "Type II" part is important. A Type I audit evaluates whether the right controls exist at a single point in time. A Type II audit evaluates whether those controls actually worked, consistently, over a sustained period. It's the difference between checking that a fire extinguisher is on the wall versus confirming that the fire safety system has been operational and tested for months.
Claimable is SOC 2 Type II certified as of January 2026.
For context, many healthcare providers' offices — the doctor you visit, the urgent care you trust — are required to meet HIPAA standards but do not typically undergo SOC 2 audits. Claimable meets both.
How your data is actually protected
Without getting deep into technical jargon, here's what's happening behind the scenes when you use Claimable.
Your data is encrypted in transit and at rest. "In transit" means while it's being sent between your device and our servers — it's scrambled so that even if someone intercepted it, they couldn't read it. Claimable uses TLS 1.3+, the latest standard for this. "At rest" means while it's stored on our servers, it's encrypted using AES-256, the same standard used by banks and government agencies.
Access to your data within Claimable is restricted by role-based controls. Not everyone on the team can see everything. Access is limited to what's necessary for the function someone performs, and every access requires two-factor authentication.
All activity is logged and monitored. If someone accesses data, there's a record of it. Those activity logs are even accessible to you directly in the Claimable app, so you can see what's happening with your case.
Claimable's infrastructure runs on AWS with multi-layered security including firewalls and intrusion detection. The company conducts annual penetration testing — where security professionals actively try to break in — and maintains an incident response plan with a 72-hour notification commitment.
Other data we collect: Why Claimable asks about your daily life, work, and finances
In addition to medical records and details about your history, Claimable's questionnaire asks about things that might not seem like typical health data: how your condition affects your daily routine, your ability to work, your relationships, and your financial situation.
There's a specific reason for this. A strong appeal doesn't just cite clinical studies and legal standards: it tells the story of what the denial actually means for you as a person. Insurers review appeals, and the human reviewers reading them need to understand the real-world consequences of withholding coverage, not just the clinical justification for the treatment.
When you share that you've had to stop working because your condition makes it physically impossible to do your job, or that routine tasks like cooking and grocery shopping have become painful or impossible, that information becomes part of your appeal's narrative argument. It demonstrates functional impairment and medical necessity in concrete, specific terms that a clinical summary alone can't convey.
This personal context is subject to the same protections as every other piece of data Claimable handles: encrypted, access-controlled, and used exclusively to build your appeal. We collect only the data we need to build a strong appeal, and it goes nowhere else.
What Claimable does NOT do with your data
This is as important as what we do. Claimable does not sell your data. Not to advertisers, not to data brokers, not to anyone. Your health information is not used for marketing or ad targeting. It's fully de-identified and aggregated when we look at things like denial rate trends, and isn’t shared with any third parties.
Claimable's AI uses your case information to build your appeal — and that's it. The system doesn't make medical diagnoses, doesn't recommend treatments, and doesn't share your information outside the scope of your specific case.
You stay in control
Claimable operates on a human-in-the-loop model. The AI generates your appeal based on your case details and the relevant evidence, but you review the final document before anything is submitted. You see exactly what's being sent, to whom, and why. If something doesn't look right, you flag it.
This isn't a system that takes your data and does something opaque with it behind closed doors. You're involved at every decision point, and you can see what's happening with your case through your Claimable account at any time.
Questions you should ask any platform
We'd encourage you to apply the same scrutiny to every service that handles your health data. When evaluating any platform — especially one that uses AI — ask: Are they HIPAA compliant, and has it been independently verified? Do they have SOC 2 Type II certification? What do they do — and not do — with your data? Who has access, and is there an audit trail?
And just as importantly: how does their AI actually work? Is it a wrapper on top of ChatGPT or another general-purpose language model, or have they built a custom system designed specifically for the task?
A general-purpose AI generates responses from broad internet training data, which means your health information may be processed in ways that aren't purpose-built for privacy or accuracy. A custom-built system like Claimable's uses retrieval-augmented generation from curated, verified sources, so your data is used to build your appeal and nothing else.
Those are the right questions. And we're glad to answer every one of them.
For a deeper look at how Claimable's AI works and why it's uniquely suited to insurance appeals, read our companion post: How Claimable's AI works for patients
If you've been denied coverage for a medication or procedure, start your appeal here.
Download a winning sample appeal
Want to see what it takes to successfully overturn a health insurance denial? Download our sample appeal to learn how we build strong, evidence-based cases that get results.
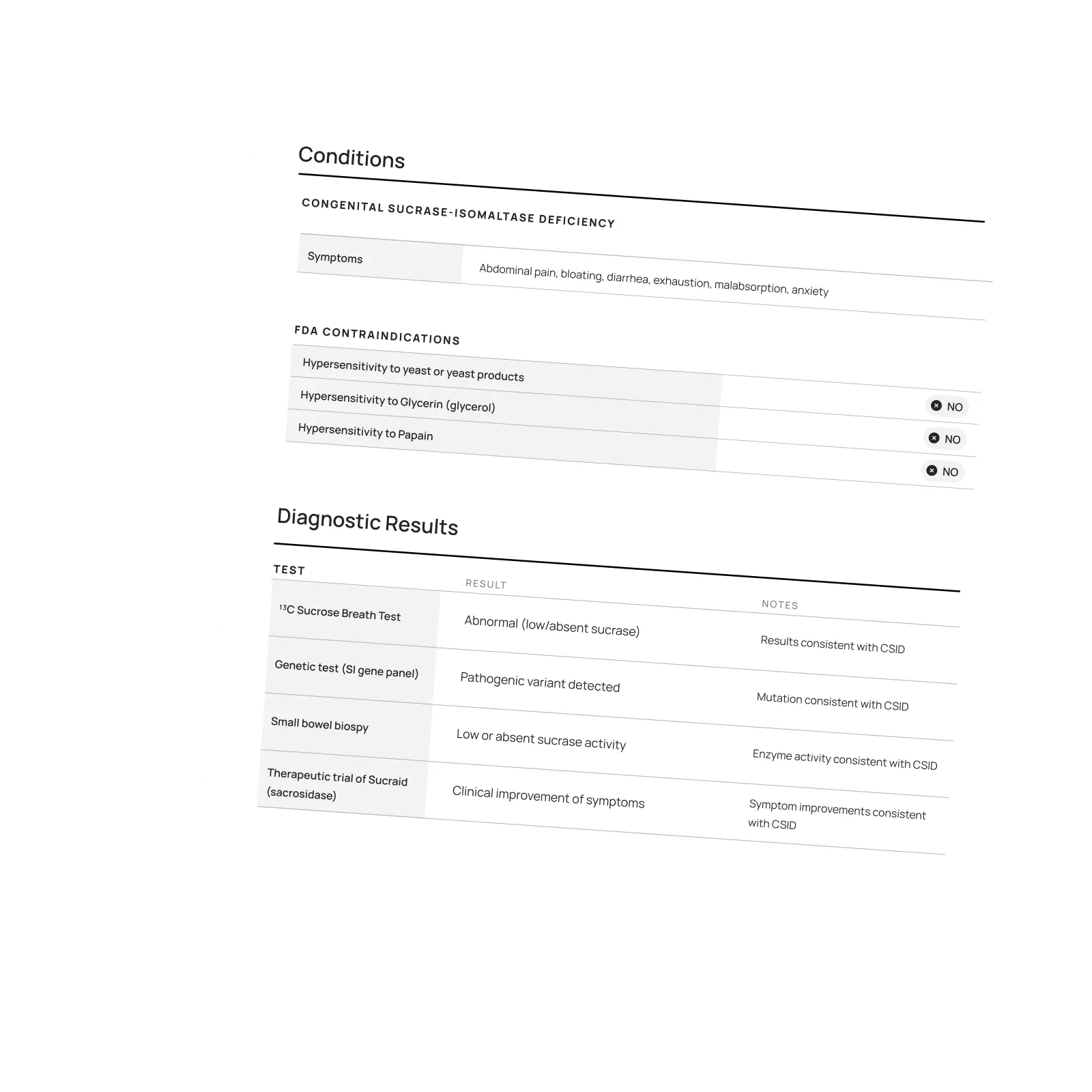
///////////////////////////////////////////////////////////////////////
//////////////////////////////////////////////////////////////////////////
////////////////////////////////////////////////////////////////////
/////////////////////////////////////////////
Each month, I endure about eight major episodes, each one leaving me exhausted, unable to concentrate, and too unwell to take part in daily life.
The frequency and unpredictability of these symptoms have isolated me socially and limited my capacity to take part in activities most people take for granted.
///////////////////////////////////////////////////////////////////////
//////////////////////////////////////////////////////////////////////////
////////////////////////////////////////////////////////////////////
/////////////////////////////////////////////
Featured stories

Be the first to know
Get the latest updates on new tools, inspiring patient stories, expert appeal tips, and more—delivered to your inbox.
You're on the list!

One of our core principles is to help patients protect their rights and level the playing field with their insurance company. This includes rights to multiple appeals, fair reviews, decision rationale, exceptions when needed, and adequate network access, among others. For more, read our post on patients rights.
For many medications, there's no cost to use Claimable to appeal for qualifying patients – thanks to our network of support partners working to expand access to care.
If you aren't eligible for a no cost appeal, Claimable charges a flat fee of $39.95 + shipping. One simple, straightforward price – no success fees or hidden charges. If appealing with Claimable is unaffordable for you, visit our nonprofit partner Coverage Fund.
Check how much Claimable will cost for your specific situation by starting an appeal and entering your insurance information. So you always know what to expect ahead of time – no surprises.
Claimable’s AI-powered platform analyzes millions of data points from clinical research, appeal precedents, policy details, and your personal medical story to generate a customized appeals in minutes. This personalized approach sets Claimable apart, combining proprietary and public data, advanced analysis and your unique circumstances to deliver fast, affordable, and successful results.
We currently support appeals for over 85 life-changing treatments. Denial reasons may vary from medical necessity to out of network, and we even cover special situation like appealing plans that won’t count your copay assistance towards your deductible (hint: those policies were banned at the federal level in 2023). That said, we are rapidly growing our list of supported conditions, treatments and reasons. You can quickly check eligibility and ask to be notified when your interest becomes available. It helps us know where to focus next 🙂
We think about appeal times in a few ways. First, many professional advocates and experienced patients spend 15, 30 or even 100 hours building an appeal–but with Claimable, this takes minutes. We automate the process of analyzing, researching, strategizing and wordsmithing appeals. Next, there is the process of figuring out where you will send it (hint: expand your reach beyond appeal departments), then printing, mailing and/or faxing your submission. We handle that, too. Finally, there is the time it takes to get a decision. We request urgent reviews when appropriate, and typically receive standard appeal decisions within a couple weeks.
Review periods are mandated by applicable laws, from 72 hours for urgent, 7 days for experimental, 30 days for upcoming and 60 days for received services. Our goal is to get a response as fast as possible, since most of our clients are experiencing long care delays or extreme pain and suffering.
Claims are denied for a variety of reasons, many of which blur definitions. We focus on helping people challenge denials by proving care is needed and meets clinical standards, in addition to addressing specific issues like experimental treatments, network adequacy, formulary or site of care preference exceptions. We don't support denials for administrative errors or missing information, as we think those are best handled by simply resubmitting the claim in partnership with your provider. That said, many of our most rewarding successes have been cases previously though 'unwinnable', with providers and patients who fought tirelessly for months without appropriate response or resolution.
A denial letter is a formal notice from your insurance company explaining why a claim was denied and how you can appeal the decision. Sometimes the notice is included within an Explanation of Benefits. It is a legal requirements; if you didn’t receive one, contact your insurance company.
A letter of medical necessity is a statement from your doctor justifying why a specific treatment is critical to your care and/or urgently needed. You can attach it to your patient appeal to strengthen your case, especially if you are requesting an urgent appeal or need to skip standard ‘step therapy’ requirements. That said, we don’t require them and are often successful without them.
A claim file contains all the documents and communications your health plan used to decide whether to approve or deny your claim. Most health plans are legally required to share this information upon request. According to a ProPublica investigation, reviewing your claim file can help expose mistakes or misconduct by your health plan, which can make your appeal stronger.
Your insurer is required by law to give you written information about how to appeal, including the name of the company that reviewed your claim and where to send your appeal. Your health insurer may work with other companies, such as Pharmacy Benefit Managers (PBMs), Third-Party Administrators (TPAs), or Specialty Pharmacies, to manage your claims. These companies might be responsible for denying your claim and handling the appeal process on behalf of your insurer.
If you don't win your first appeal– don't give up! Many people are successful on their 2nd, 3rd or even 4th try, and future appeals are reviewed by independent entities. That said, we wrote a whole guide to understanding your options, including escalating your appeal and seeking other assistance for covering costs, forgiving debt or even seeking legal or regulatory support.
While both denial rates and appeal success rates vary widely by the type of health plan, state, and insurance company, studies have shown more than 50% of people win their appeal–and we apply strategies to boost your chances of success. Claimable has an 80% appeal success rate. The biggest denial challenge is that most people never appeal–allowing unjust denials to control their healthcare options because they are unaware of their rights or lack the support needed to fight back. No one needs to fight alone–Claimable is here to help. We know first hand that many denials are based on errors, inconsistencies or auto-decisions, and have proven strategies for fighting back against this injustice.
Let’s get you covered.

